No products in the cart.

Is a pt 141 nasal spray a legitimate research tool, or is it just a convenient label attached to an unapproved format of bremelanotide?
That’s the question most buyers skip. They focus on delivery convenience and forget the more important distinction: bremelanotide exists in both an FDA-approved injectable form and a separate intranasal research and compounding field. If you’re evaluating PT-141 for laboratory, analytical, or preclinical work, that difference changes how you interpret study data, compare formulations, document procurement, and manage experimental consistency.
Bremelanotide is a melanocortin receptor agonist. A practical way to think about it is as a key that can fit several related receptor “locks” in the central nervous system, rather than a simple peripheral delivery agent. That central mechanism is why the compound continues to attract interest in arousal-pathway research, and why route of delivery matters so much in study design. If you need a broader primer before going deeper, PepFlow’s guide on what are peptides is a useful refresher.
This briefing approaches PT-141 nasal spray the way a lab director would. It focuses on pharmacology, historical intranasal evidence, formulation trade-offs, handling controls, dosing logic for research settings, and the regulatory line between a research-grade nasal spray and the approved injectable product.
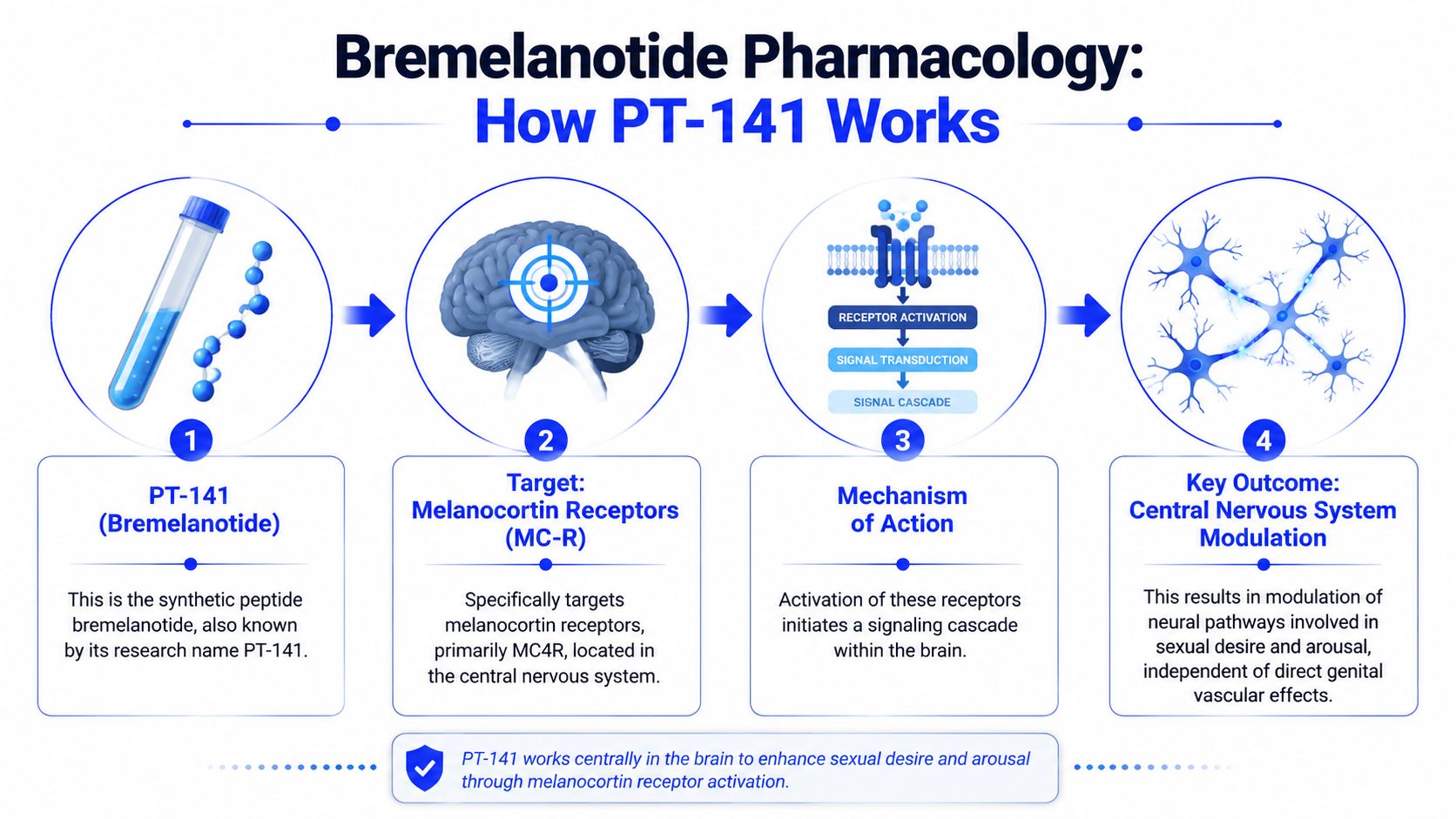
PT-141 is the research name for bremelanotide, a synthetic peptide studied for its central melanocortin activity. In peptide research circles, the nasal format gets attention because it offers a non-injectable route, but that convenience has to be weighed against formulation variability, route-dependent absorption, and regulatory confusion.
A lot of online content blurs those categories. It treats intranasal PT-141 like another standard commercial dosage form. It isn’t. The better way to approach it is as a research and compounding format that sits apart from the approved injectable product.
For laboratories, that distinction drives practical decisions:
Practical rule: If your records don’t separate “approved injectable bremelanotide” from “research-grade intranasal PT-141,” your downstream conclusions can get muddy fast.
Why does route of administration matter so much with PT-141 if the active compound is the same? Because bremelanotide is defined less by local tissue exposure and more by its central melanocortin receptor activity, and that creates real differences between a research-grade nasal preparation and the FDA-approved injectable product.
Pharmacologically, PT-141 is a synthetic melanocortin receptor agonist with activity centered on receptor systems involved in sexual arousal signaling in the central nervous system. That is the key starting point for study design. Investigators who frame bremelanotide as a simple blood-flow agent can select the wrong endpoints, overinterpret peripheral readouts, or compare intranasal and subcutaneous data as if they were interchangeable.
The receptor picture is also broader than a single highly isolated target. Bremelanotide has been studied primarily for melanocortin receptor activity, especially MC4R-related effects in sexual-function research, which helps explain why outcome measures often differ from studies built around vasodilatory mechanisms or direct smooth-muscle pharmacology (PubMed overview of bremelanotide pharmacology).
That distinction is practical, not academic.
Intranasal development drew attention because it offered a non-injectable route for on-demand administration, but that convenience came with a different set of experimental constraints. Nasal delivery introduces formulation-dependent absorption, administration-technique variability, and greater uncertainty when researchers try to compare exposure with the approved subcutaneous product.
That is where many summaries lose precision. Vyleesi, the FDA-approved bremelanotide product, is an injectable formulation with reviewed manufacturing, labeling, and pharmacokinetic data tied to that route of administration (FDA prescribing information for Vyleesi). By contrast, PT-141 nasal spray discussed in research settings has generally referred to investigational, compounded, or otherwise non-approved intranasal preparations. For procurement, recordkeeping should treat those as different material categories, even when the peptide identity is nominally the same.
A PubMed-indexed crossover study illustrates why the nasal route stayed under review. In that trial, 19 men received 7.5 mg intranasal PT-141 plus 25 mg sildenafil versus sildenafil with placebo spray, with erectile activity measured over a 6-hour post-dose window using RigiScan during visual sexual stimulation. The combination produced a significantly greater erectile response than sildenafil alone and was reported as safe and well tolerated in that study (PubMed study on intranasal PT-141 with sildenafil).
For laboratory planning, the main lesson is straightforward. Keep the mechanism, the dosage form, and the regulatory status in separate columns of your notes. If those categories get merged, teams can end up citing approved-injection data to justify a research nasal spray protocol, and that is a documentation error before it becomes a scientific one.
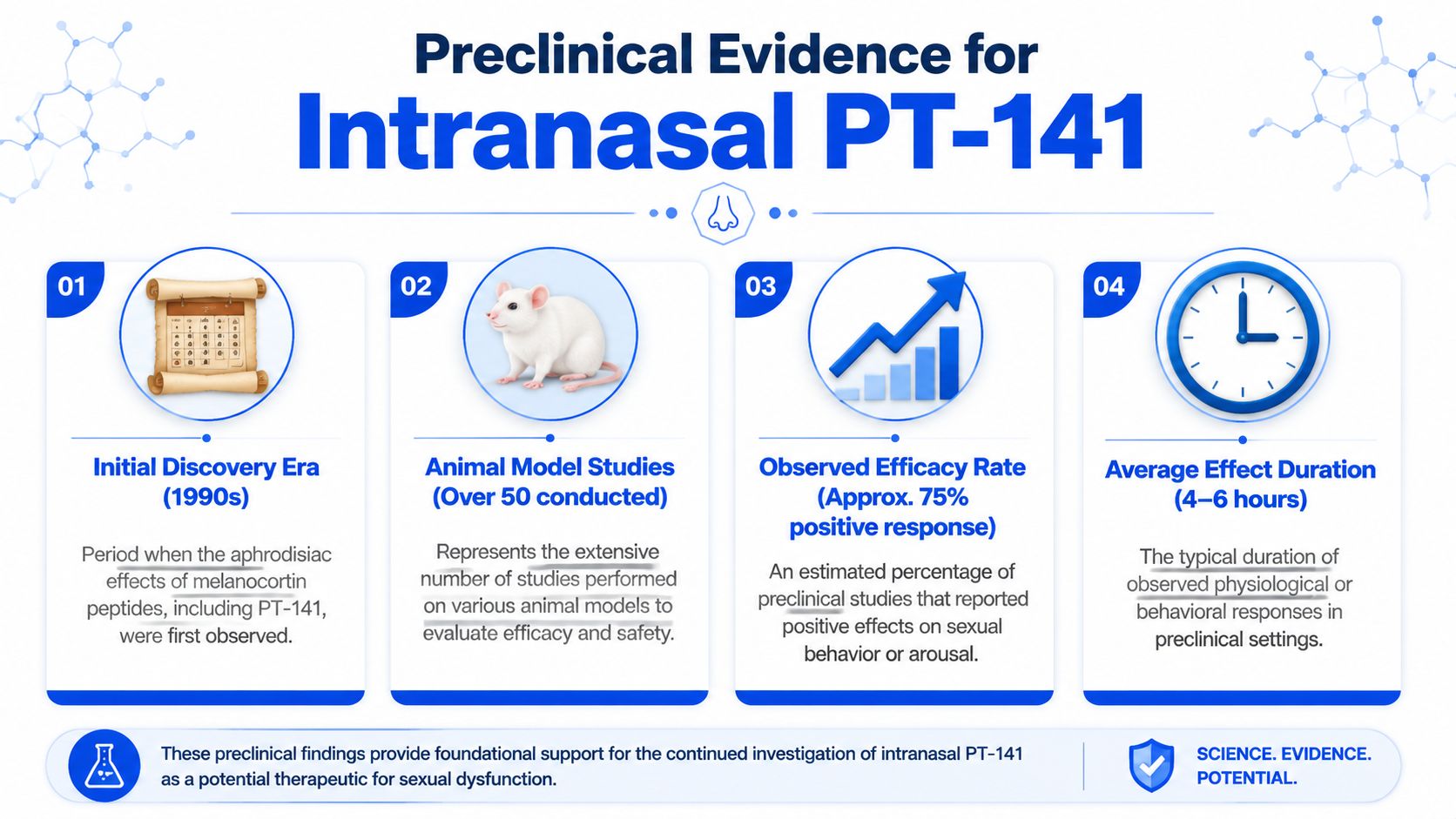
For a laboratory team, the preclinical and early clinical record on intranasal PT-141 is useful for one reason. It helps define whether the nasal route should be treated as a serious delivery model with its own variables, or merely as an informal substitute for the approved injection. The record supports the first view.
Earlier work in men’s sexual-function research showed a pharmacologic signal with intranasal administration, including interest in pairing the peptide with sildenafil. As noted earlier, that finding is enough to justify route-specific study design. It is not enough to justify assuming that a research nasal spray and FDA-approved subcutaneous bremelanotide can be interpreted under the same exposure framework.
A better reading of the evidence focuses less on headline efficacy and more on operational limits. Intranasal peptide delivery introduces extra sources of variance before any outcome measure is collected. Spray angle, atomizer output, residual volume in the device, nasal mucosal condition, and timing relative to congestion or rhinitis all affect delivered dose. In a procurement or protocol review, those are not minor details. They determine whether two nominally identical PT-141 nasal preparations can be expected to behave similarly in vivo.
Published comparisons between nasal and injectable PT-141 commonly describe the nasal route as less predictable and often less dose-efficient than subcutaneous administration (route comparison for PT-141 nasal spray vs injection). That distinction matters most at the protocol and documentation level.
The approved injectable product exists within a reviewed manufacturing and labeling framework. Research-grade nasal spray usually does not. A lab therefore has to document more than peptide identity. It has to document formulation vehicle, concentration, device performance, route-specific administration instructions, and the basis for any chosen dose range. If those records are incomplete, interpretation becomes weak even when the underlying compound is correct.
| Research issue | Intranasal PT-141 | Subcutaneous bremelanotide |
|---|---|---|
| Administration | Needle-free, but technique-sensitive | Procedural, but easier to standardize |
| Absorption | Affected by mucosal condition and spray performance | Usually more predictable |
| Dose planning | Requires route-specific justification | Can be anchored to a fixed delivered volume |
| Documentation burden | Higher, because formulation and device details affect exposure | Lower, because delivery is easier to verify |
In practice, intranasal PT-141 is most defensible when the route itself is part of the research question. It is a weaker choice when the goal is tight exposure control or direct comparison to the FDA-approved injectable form without route-matched controls.
The first question is simple. What, exactly, is being delivered with each spray?
For PT-141 nasal work, concentration alone is an incomplete specification. A bottle labeled 1 mg/mL, 2 mg/mL, or 10 mg/mL only identifies peptide strength in solution. It does not establish the mass delivered per actuation, the droplet profile reaching the nasal mucosa, or the extent to which the vehicle supports peptide stability during routine use. Those details matter more with intranasal material than with the FDA-approved injectable bremelanotide product, where dose is tied to a defined injection format and a regulated finished drug configuration.
Compounding references commonly describe PT-141 nasal preparations across a range of concentrations, including formulations such as 20 mg in 10 mL, which corresponds to 2 mg/mL. Pharmacy-facing descriptions also present dosing in sprays rather than milligrams, which is the practical problem a lab has to solve before study start (Bremelanotide 20mg/10mL Nasal Spray formulation listing). A spray count is not a dose unless the pump output has been measured and the formulation concentration has been confirmed against batch records.
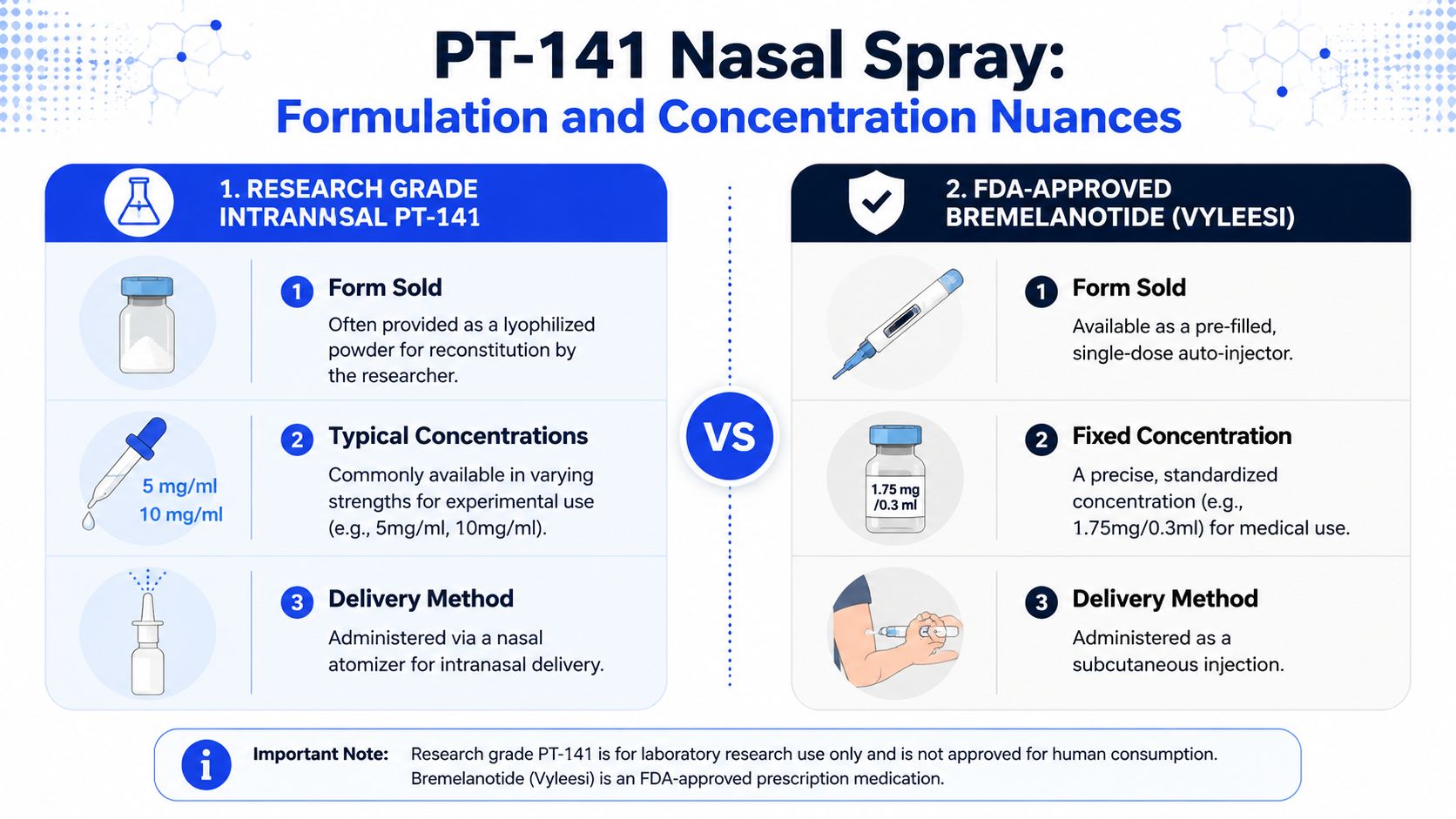
A second distinction is formulation intent. Research-grade PT-141 nasal spray may be assembled for exploratory use, analytical method development, or route feasibility work. The FDA-approved injectable form was developed, reviewed, and labeled as a finished subcutaneous product. Those are different regulatory categories with different documentation burdens. If procurement records only capture peptide identity and bottle strength, the lab still lacks the route-specific data needed to defend exposure assumptions.
Before any nasal batch enters active use, review it at three levels:
Solution composition
Record stated concentration, total fill volume, excipient system, pH if available, and whether the material was compounded externally or prepared under an internal SOP.
Device performance
Record pump manufacturer or device type, nominal spray volume, priming instructions, and any bench verification of delivered output across repeated actuations.
Route suitability
Confirm that the formulation is intended for intranasal administration rather than simple peptide dissolution. A clear solution is not enough. Viscosity, tolerability, and spray behavior affect whether the preparation can function as a reproducible nasal product.
Labs often miss the device piece.
I treat the atomizer, bottle, and solution as one administered system because any one of them can shift delivered dose. Two bottles with the same stated concentration can produce meaningfully different exposure conditions if pump output or plume quality differs. That is one of the main practical differences between research-grade nasal PT-141 and the approved injectable comparator.
If a lab is receiving pre-made PT-141 nasal spray or preparing a batch in-house for nonclinical work, these controls improve interpretability:
Verify concentration against source records
Match the label claim to the certificate, compounding record, or internal preparation sheet before first administration.
Measure delivered volume per actuation
Do not assume the nominal pump specification reflects real output after shipping, storage, or repeated use.
Document priming status
First sprays, re-primed sprays, and routine sprays may not deliver the same volume.
Fix the administration script
Keep head position, number of sprays, interval between sprays, and nostril assignment constant within the protocol.
Separate bottle strength from administered mass
Batch files should state both concentration in mg/mL and estimated mass per spray based on verified output.
Route-dependent variability is the cost of using a nasal system. If the study needs a needle-free intranasal model, that trade-off may be justified. If the goal is tight alignment with the FDA-approved bremelanotide exposure model, the injectable form remains easier to standardize and easier to defend in regulatory or audit review.
PT-141 is easy to mishandle if the lab treats it like a casual stock solution. For peptide work, stability control starts at receipt, not at first use.
For lyophilized material, keep the vial in a cool, dry, dark environment with tight inventory control. Minimize repeated temperature cycling, and document when the vial is removed, opened, and re-sealed. If the material is reconstituted for analytical or preclinical work, use a sterile process and assign an internal beyond-use window based on your lab’s SOP and stability policy.
For pre-made intranasal sprays, protect the formulation from unnecessary light and heat exposure, and avoid repeated uncontrolled transport between storage locations. The bottle, pump, and solution should be treated as one unit. Once a spray enters active use, track every handling event that could affect output consistency.
A good batch record for PT-141 nasal spray should include more than lot and date. At minimum, capture:
Identity details
Compound name, internal code, supplier, lot number, and received condition.
Form factor
Lyophilized peptide, prepared solution, or assembled nasal spray.
Preparation record
Reconstitution solvent, date, preparer initials, and final target concentration if prepared in-house.
Storage log
Assigned storage condition, movement history, and discard or review date.
Device traceability
Spray bottle or atomizer identifier if the route is intranasal.
Store the material one way. Document it another way. Both matter. If only one is done well, the record still fails.
Labs also benefit from a deviation log. If a bottle was left out, re-primed mid-study, or transferred into a different device, that should be recorded immediately. Most peptide variability problems aren’t mysterious. They usually trace back to weak documentation.
How should a lab set dose levels for PT-141 nasal spray without blurring the line between a research intranasal product and the FDA-approved injectable form of bremelanotide? Start by treating those as separate exposure systems with different formulation, delivery, and documentation demands.
Dose planning around PT-141 often becomes unreliable because three things get mixed together. Research-grade nasal spray concentrations, historical intranasal study doses, and the approved subcutaneous Vyleesi framework are not interchangeable. A bottle label gives nominal concentration. It does not establish delivered dose, absorbed dose, or comparability to injection.
As noted earlier, intranasal PT-141 has been discussed in historical dose-finding work across a broad range. Those numbers are best used as boundary markers for study design, not as a ready-made regimen. For laboratory work, the practical question is narrower: what amount leaves the device, reaches the target surface under your administration method, and produces a measurable effect in the model you selected?
That distinction matters more for intranasal work than for injection. With the injectable product, the route and unit dose are defined by an approved presentation. With a research nasal spray, concentration, spray volume, plume quality, retention, and operator technique can all change exposure.
Build the study around delivered input, not stated concentration alone.
For in vitro work, that usually means defining the final exposure in the assay system after dilution, vehicle contribution, contact time, and any adsorption losses to tubes or plates are accounted for. For in vivo intranasal work, the record should capture target concentration, measured pump output per actuation, number of actuations, administration sequence, and whether any material loss was observed during dosing.
A useful starting framework is to match the dose plan to the study objective:
Exploratory route study
Confirm that intranasal administration can generate a detectable signal under controlled handling and a fixed administration script.
Comparative route study
Hold formulation and endpoint timing as constant as possible, then compare intranasal delivery with injectable administration as separate route conditions, not as assumed equivalents.
Formulation study
Test whether concentration, excipient system, and spray device alter output consistency or endpoint performance.
Pharmacology screening study
Use preplanned escalation steps tied to defined stopping criteria, observation windows, and endpoint collection times.
Keep escalation disciplined. If actuation count changes between cohorts, document that as a dose change. If concentration changes but the device does not deliver consistently, the study has two moving variables instead of one.
Intranasal and injectable bremelanotide differ in more than route name. They differ in how a lab controls the delivered amount.
For injectable reference work, dose accountability is usually simpler because the administered volume can be measured directly and the presentation is standardized. For PT-141 nasal spray, the device becomes part of the dosing system. Any variation in priming, bottle angle, nasal deposition, or residual fluid in the actuator can shift the practical dose even when the labeled strength stays the same.
That is why I advise labs to verify three things before a larger animal study begins:
Actuation output
Measure delivered volume across repeated sprays from the same device lot.
Operator consistency
Use one written administration procedure and qualify staff against it.
Comparator logic
If injection is the benchmark, define whether the goal is route feasibility, relative onset, or endpoint magnitude. Do not imply bioequivalence unless the study is built to test it.
A common failure point is treating a higher mg/mL label as a stronger experiment. It may only be a more concentrated bottle. If the atomizer outputs irregularly or the subject does not retain the dose well, nominal strength will overstate exposure and weaken interpretation.
Dose records should be specific enough that another team could reconstruct what was administered.
At minimum, document:
For PT-141 nasal spray, better records usually produce better data. In this area, logistical control is part of dose control.
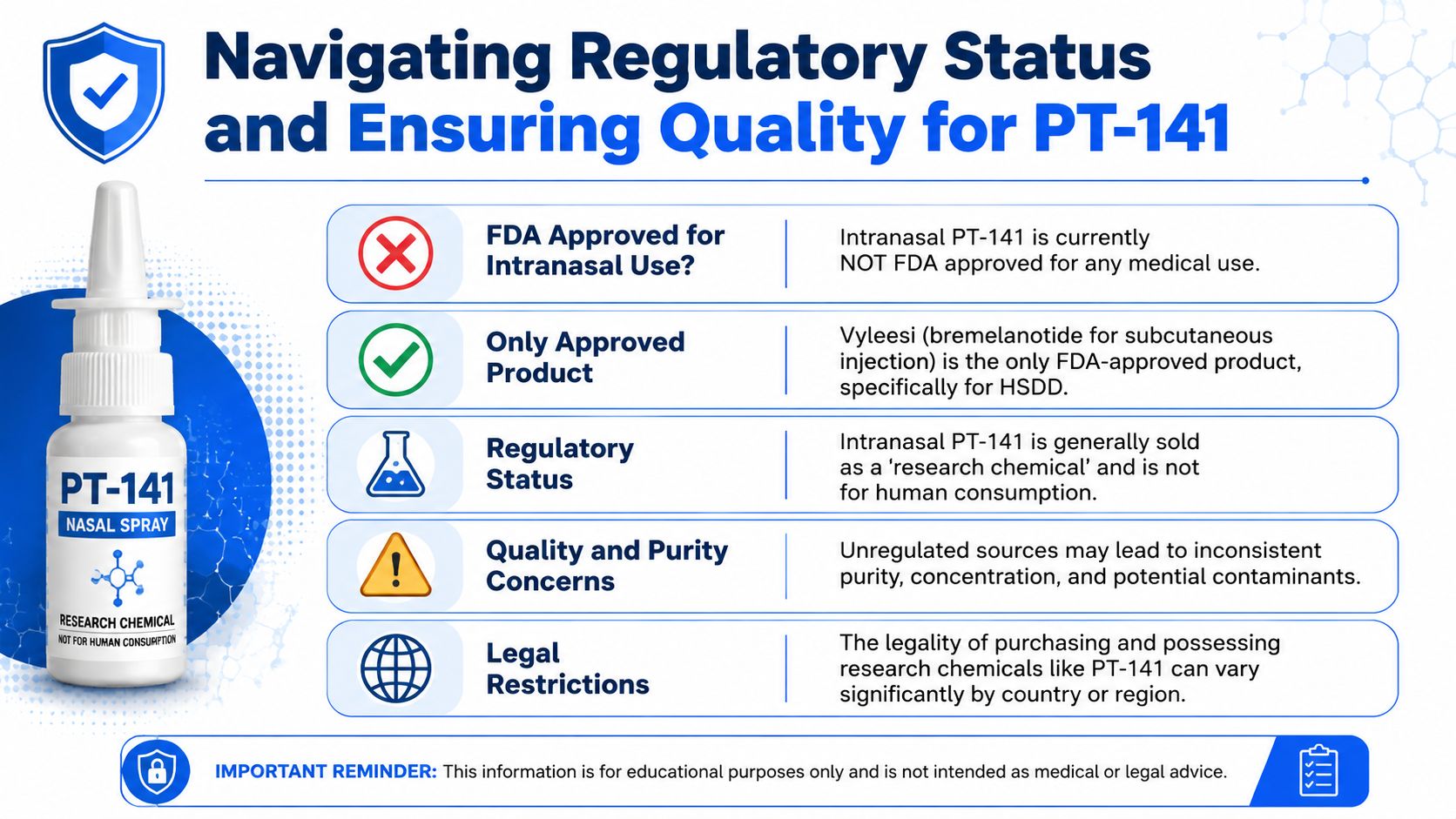
The most important regulatory point is simple. The FDA-approved bremelanotide product is injectable Vyleesi, not intranasal PT-141. Discussions that present nasal spray PT-141 as though it were a normal approved consumer therapy flatten a distinction that matters for legal, ethical, and documentation reasons.
One review notes that intranasal PT-141 research was halted in 2007 because of blood pressure concerns, and that current intranasal availability sits in the research chemical market, not as an approved therapy (regulatory overview of PT-141 and Vyleesi distinction).
That means procurement language should be precise. If a lab buys “PT-141 nasal spray,” the receiving record should not imply FDA-approved therapeutic status. It should identify the material according to its actual regulatory position in the supply chain.
Here is the regulatory snapshot in visual form.
A short explainer can help frame the distinction before procurement teams make assumptions.
Once the regulatory line is clear, quality review becomes much easier. For PT-141 nasal spray or related peptide inputs, I’d expect a supplier review process to include the following:
Certificate of Analysis
Confirm the lot has a traceable COA tied to the exact batch being sold.
Third-party testing scope
Purity documentation matters, but so do contamination controls. If the supplier claims microbial or endotoxin testing, those reports should be available for the same lot.
Manufacturing claims
“Made in the USA” or similar language should be backed by clear batch and sourcing documentation.
Label clarity
The product should be identified as research-use material when that is its true status.
Formulation transparency
For nasal sprays, concentration alone isn’t enough. Ask how the formulation is prepared, packaged, and lot-tracked.
Buy the paperwork before you buy the peptide. If the documentation is weak, the material is weak for research purposes even when the label looks polished.
pt 141 nasal spray remains a useful research format, but only when it’s handled as a distinct intranasal strategy rather than a casual substitute for injectable bremelanotide. The critical points are straightforward: understand the melanocortin mechanism, respect route-specific variability, document formulation and device factors carefully, and keep the regulatory distinction clear. Good PT-141 work depends less on hype and more on tight handling, lot traceability, and disciplined protocol design.
If you need a reliable source for laboratory and analytical peptide procurement, Peptide Warehouse USA offers research-use compounds with transparent batch documentation, including COAs and supporting quality records. Explore their catalog or learn more about their quality standards if you’re comparing suppliers for PT-141 and related peptide research materials.



