No products in the cart.

Why are so many people asking about peptides for thyroid support when the actual human evidence is still so limited?
That gap matters. Interest has grown because peptides are a real and important drug class in modern medicine, and thyroid biology includes peptide signals that are already well understood. But “peptides for thyroid” can mean very different things: upstream signaling compounds, immune-modulating research tools, or broad tissue-repair claims that get bundled into thyroid discussions without strong thyroid-specific data.
The useful question isn’t whether peptides sound promising. It’s which mechanisms make biological sense, which compounds have actual preclinical support, and where marketing has run ahead of proof. For readers trying to evaluate this area carefully, the smartest starting point is usually basic thyroid assessment and pattern recognition, not hype. If you’re comparing conventional workup pathways, these UK private thyroid screening options give a practical overview of what thorough thyroid testing can look like.
What follows is a research-based guide for knowledgeable non-specialists. It separates mechanism from evidence, shows where the field is strongest, and explains why thyroid peptide research still sits much closer to hypothesis generation than established clinical use.
Interest in peptides for thyroid health usually starts with a reasonable idea. The thyroid is controlled by peptide signals, autoimmune thyroid disease involves immune dysfunction, and peptide therapeutics have become a major part of modern pharmacology. That combination makes the field sound more mature than it is.
The problem is that mechanism and proof aren’t the same thing. A compound can fit neatly into thyroid physiology on paper and still lack controlled human data. That’s especially important in thyroid research, where people often mix together endocrine signaling, inflammation, tissue repair, and general wellness under one label.
Core distinction: A plausible mechanism tells you where to investigate. It doesn’t tell you that a treatment works in humans.
There’s also a category error that shows up often online. Some discussions refer to peptide hormones that naturally regulate the hypothalamic-pituitary-thyroid axis. Others jump to synthetic analogs, complex gland-derived mixtures, or non-thyroid peptides proposed to influence inflammation or recovery. Those aren’t interchangeable.
A more disciplined way to think about the topic is to split it into three questions:
That framework leads to a more useful conclusion than the usual “promising” language. Some peptide ideas for thyroid disease are biologically coherent and worth studying. Very few have crossed the line into proven thyroid therapy.
The thyroid doesn’t act alone. It works inside a layered feedback circuit that links the brain, pituitary, and thyroid gland. If you don’t understand that control system, claims about peptides become hard to evaluate.
A home thermostat is a useful analogy. The hypothalamus acts like the control center that detects when more output is needed. It releases TRH, or thyrotropin-releasing hormone, which signals the pituitary. The pituitary then releases TSH, or thyroid-stimulating hormone, which tells the thyroid gland to produce thyroid hormones.
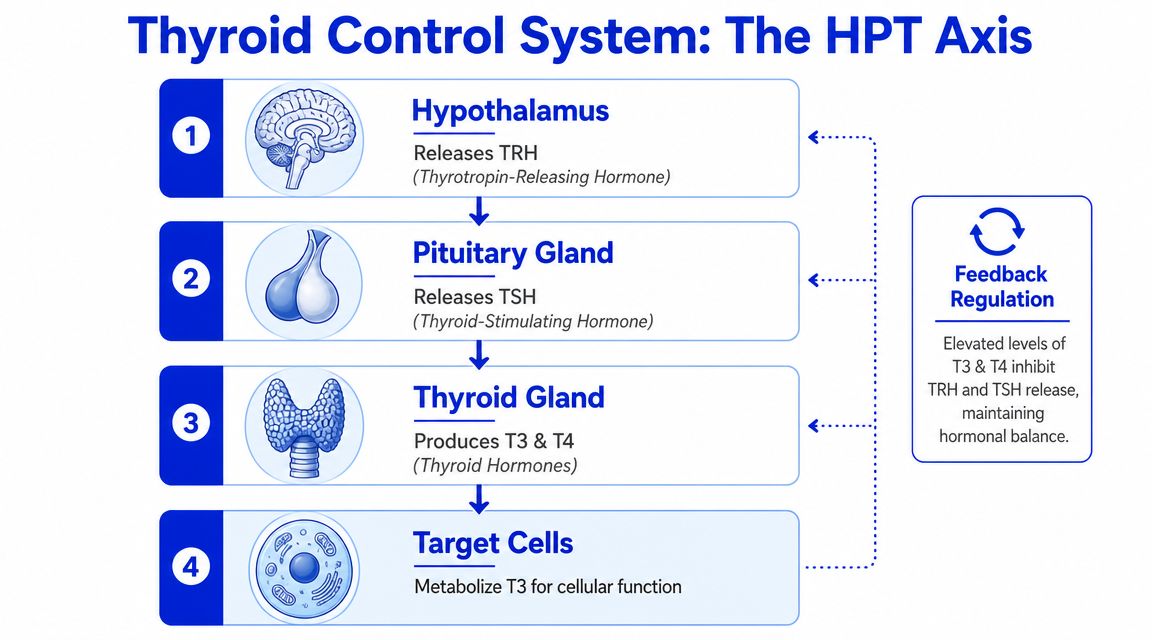
When circulating thyroid hormone is adequate, the brain and pituitary reduce the signal. When thyroid hormone is low, signaling tends to increase. This feedback loop is why upstream peptide biology matters in thyroid research. A peptide can potentially act at the level of hypothalamic signaling, pituitary stimulation, immune regulation, or tissue response.
TSH is the command signal. It doesn’t do the thyroid’s metabolic work itself. Instead, it instructs the gland to synthesize and release hormone.
The thyroid mainly produces T4 and a smaller amount of T3. T4 is often described as a prohormone or reservoir form, while T3 is the more active form at the cellular level. Peripheral tissues can convert T4 into T3, which is one reason local regulation matters and why some peptide theories focus beyond the gland itself.
A few practical points help make sense of research claims:
A peptide claim aimed at the thyroid should always answer one basic question: where in the control system is it supposed to act?
That question filters out a lot of vague marketing. If a compound doesn’t have a clear place in the HPT axis, peripheral hormone handling, or immune pathophysiology, the thyroid relevance may be more speculative than substantive.
The phrase peptides for thyroid sounds singular, but the biology points to several very different routes of action. Grouping them together hides the underlying scientific issue. The mechanisms don’t ask the same question, and they shouldn’t be judged by the same standard.

The most straightforward mechanism involves TRH biology. TRH is a native peptide signal released by the hypothalamus. Its role in stimulating the pituitary is well established. That makes it a natural conceptual starting point for thyroid peptide discussions.
But there’s an important limit here. Understanding endogenous TRH doesn’t mean that giving exogenous peptide support improves thyroid outcomes in humans. Mechanistic legitimacy is not clinical validation. This distinction often blurs many conversations, especially when people move from “TRH matters” to “therefore peptide supplementation should help.”
A second pathway is more indirect. Researchers sometimes consider whether peptides could influence the local handling of thyroid hormone, including the conversion of T4 to T3 in peripheral tissues. In principle, this matters because thyroid status isn’t determined only by gland output. It also depends on how tissues activate, deactivate, transport, and respond to hormone.
This is a useful research lens, but it’s also where claims can become too broad. If a peptide affects inflammation, stress signaling, tissue turnover, or repair pathways, that doesn’t automatically mean it has a defined or beneficial effect on thyroid hormone conversion. Any such hypothesis has to be tested through specific assays, not inferred from general biological activity.
Here’s a concise video overview that helps anchor the broader hormone signaling context before jumping to conclusions about interventions.
The third pathway is the most compelling from a disease-model perspective. Many important thyroid disorders are autoimmune. That changes the question from “Can a peptide stimulate thyroid hormone production?” to “Can a peptide alter the immune process driving thyroid injury or receptor stimulation?”
This distinction is critical. In autoimmune thyroid disease, the main target may not be the gland’s hormone-making machinery itself. The target may be antibody production, immune-cell behavior, receptor interaction, or downstream tissue remodeling.
That’s why the strongest thyroid-specific peptide signal so far has come from an autoimmune Graves’ model rather than from general hypothyroid optimization claims. In that line of work, the peptide isn’t just being treated as a generic wellness compound. It’s being used as a targeted immunologic intervention.
Research lens: For thyroid peptides, immune modulation is often more scientifically coherent than vague “boost the thyroid” language.
Which peptides have a plausible thyroid mechanism, and which are mostly being pulled into the conversation by association?
That distinction matters because “peptides for thyroid” is not a single research category. It includes endogenous hypothalamic signals, synthetic analogs built to alter receptor behavior, and general experimental peptides that are discussed in thyroid contexts because immunity, tissue injury, or endocrine cross-talk may be involved. Grouping them together obscures the main scientific question. A coherent mechanism does not equal a validated thyroid application.
The clearest way to compare these compounds is to separate mechanistic plausibility from direct thyroid evidence.
| Peptide | Proposed Mechanism | Primary Research Area | Level of Evidence |
|---|---|---|---|
| TRH | Central endocrine signaling through the hypothalamic-pituitary-thyroid axis | Hormonal regulation and upstream signaling | Established biology, but not proof of peptide supplementation as thyroid treatment |
| TRH analogs such as taltirelin | Modified signaling at TRH-related pathways | Neuroendocrine and signaling research with theoretical thyroid relevance | Mechanistic relevance, thyroid-specific application remains limited |
| Cyclic TSH receptor mimetic peptides | Immune modulation directed at receptor-related autoimmune activity | Graves’ disease and orbitopathy models | Preclinical thyroid-specific signal in animal research |
| Epitalon | Proposed systemic regulatory and endocrine effects | Broad experimental anti-aging and endocrine hypotheses | Thyroid-specific evidence remains unproven |
| BPC-157 | Proposed tissue repair and inflammation-related effects | General repair and inflammatory research, not thyroid-specific proof | Indirect theoretical relevance only |
A useful pattern appears once the categories are separated this way. The compounds with the strongest thyroid-specific rationale are often the least suitable for broad consumer-style claims, because their relevance is tied to narrow disease mechanisms rather than general thyroid “support.”
TRH matters because it is part of the normal control loop for thyroid function. That makes it biologically central, but the inference many readers want to make is still unsupported. Knowing that TRH regulates the axis does not show that giving a peptide externally improves thyroid outcomes in a meaningful clinical setting.
TRH analogs, including taltirelin, test a more specific idea. Researchers are asking whether modified peptide signaling can change downstream neuroendocrine behavior in useful ways while altering stability, receptor interaction, or pharmacokinetics relative to native TRH. That is a legitimate mechanistic research program. It is still a long distance from evidence that these compounds treat hypothyroidism, autoimmune thyroid disease, or other common thyroid disorders.
Cyclic peptides based on the TSH receptor are the most thyroid-focused group in the current literature. Their logic is more precise than “supporting the gland.” They are designed to interfere with the autoimmune process directed at the TSH receptor, which is why they have been studied in Graves’ disease models rather than in vague wellness frameworks. In a well-known mouse study of Graves’ disease and orbitopathy, peptide treatment was associated with lower TSHR-binding antibodies and improvement in several disease features, including thyroid and orbital changes. That is a meaningful preclinical signal because the outcomes were thyroid-specific and disease-specific. It still remains preclinical evidence, not a basis for human therapeutic conclusions. Readers who want a better framework for judging studies of this kind can use this master scientific paper analysis.
Epitalon sits in a different category. Its online reputation often comes from broad claims about endocrine regulation, aging, or systemic resilience. The thyroid relevance is mostly inferential. Unless a study measures thyroid-specific endpoints such as TSH, free hormones, antibodies, imaging findings, or histology, the compound remains thyroid-adjacent rather than thyroid-directed.
BPC-157 is even further from direct thyroid evidence. The proposed rationale usually runs through inflammation, mucosal integrity, or tissue repair. Those pathways could be relevant to autoimmune disease in theory, but each step adds uncertainty. A chain of plausible biological links is still weaker than direct evidence in thyroid models.
That mechanism-to-evidence gap is the central issue across this section. A peptide can have a clear biological target, a reasonable hypothesis, and interesting animal data, yet still fall short of being a credible thyroid intervention for humans.
One broader point is easy to misread. Peptide drugs are a real therapeutic class, and endocrine pharmacology has many examples of successful peptide-based medicines. That general fact does not validate thyroid-specific peptide claims. The class has clinical legitimacy. This niche remains early, fragmented, and mostly hypothesis-driven.
How much of the thyroid peptide discussion rests on demonstrated clinical benefit, and how much rests on plausible biology that has not yet been tested rigorously in humans?
That distinction matters more in this niche than in many others. Thyroid peptide claims often combine mechanistic reasoning, animal findings, and small human observations into a single narrative, even though those forms of evidence answer different questions and carry very different weights.
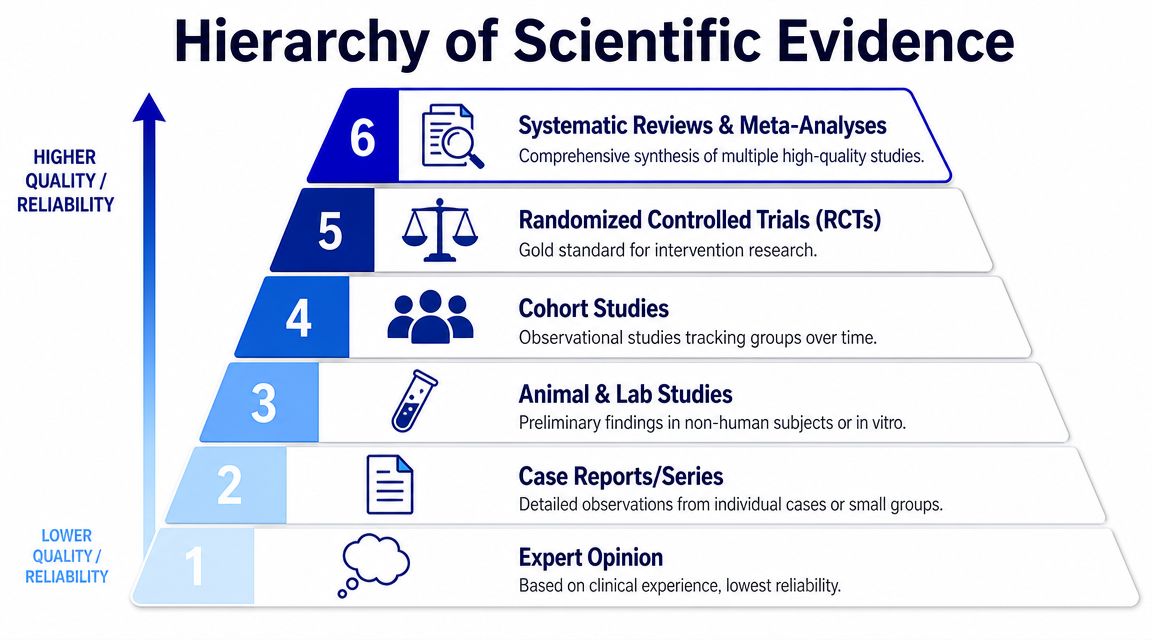
The most useful framework is still the evidence pyramid. Mechanistic studies can show receptor binding, signaling effects, or immune modulation. Animal models can test whether those effects alter thyroid histology, antibody patterns, or hormone regulation under controlled conditions. Human data must answer a different question. They have to show that a defined compound, given at a defined dose, produces a clinically meaningful thyroid-related effect under conditions that limit bias.
If you want a better framework for reading these papers critically, this master scientific paper analysis is a useful guide to study design, limitations, and what a paper can prove.
A practical screen for this literature is simple:
The current evidence base sits low on that pyramid. The most coherent signal comes from preclinical work, especially studies framed around immune regulation in autoimmune thyroid disease. That is scientifically interesting because thyroid dysfunction in these settings is not only a hormone problem. It is also an immune problem. A peptide that changes cytokine balance, antigen presentation, or lymphocyte behavior could therefore influence thyroid outcomes indirectly, even if it does not act as a classic thyroid hormone analogue.
That mechanistic logic is reasonable. The clinical proof remains limited.
For autoimmune thyroiditis and related settings, one often-cited human publication is a clinical report involving a combined thyroid and pineal peptide preparation. The report describes improvements in general condition, antibody measures, and ultrasound findings in patients with autoimmune thyroiditis. Those observations are hypothesis-generating, but they do not resolve the central questions. The preparation was a combination product rather than a single well-defined peptide. That makes it difficult to assign causality, replicate the intervention cleanly, or connect the observed effect to a specific molecular mechanism.
This is the mechanism-to-evidence gap in its clearest form.
A peptide can have a plausible target, fit current models of thyroid immunology, and produce encouraging findings in preclinical systems. None of that establishes therapeutic value in humans. To make that step, the field would need controlled trials with defined compounds, prespecified thyroid endpoints, adequate follow-up, and enough methodological detail to separate signal from noise.
The online discussion often compresses those stages into one claim. The literature does not support that compression. A cautious reading leads to a narrower conclusion. Peptides remain a credible research direction for thyroid-related biology, particularly where immune modulation is relevant, but thyroid-specific clinical application is still early, fragmented, and far from proven.
A serious discussion of peptides for thyroid has to separate research interest from medical use. That isn’t just a legal distinction. It’s a scientific one.
As of April 2026, no peptide compound had received FDA approval for any thyroid disease indication. The same review notes that TRH biology is well established, but that doesn’t justify exogenous peptide supplementation as a proven human treatment. In practical terms, thyroid-specific peptide use remains preclinical or hypothesis-generating rather than clinically settled.
That status has consequences. A research compound is not the same as a regulated thyroid medication. It hasn’t met the same standard for indication-specific safety, dosing, manufacturing consistency in medical use, or efficacy in controlled trials for thyroid disease.
People often underestimate how many variables sit between a promising mechanism and a reliable intervention. Those variables include formulation, route of administration, peptide stability, off-target effects, and whether the proposed benefit even maps to the disease mechanism in question.
For thyroid-related compounds, the risk of oversimplification is especially high because thyroid symptoms overlap with many other issues. Fatigue, weight change, hair changes, mood shifts, and cold intolerance aren’t specific enough to validate a peptide hypothesis on their own.
A responsible research posture includes a few basic rules:
Practical rule: If a thyroid peptide claim depends more on testimonials than on defined endpoints and controlled data, it belongs in the hypothesis column, not the treatment column.
In laboratory settings, peptide quality isn’t a minor procurement detail. It directly affects whether a thyroid experiment answers the intended question or produces noise.
A useful sourcing checklist starts with documentation, not branding.

Researchers should look for:
The point isn’t just compliance. It’s interpretability. If peptide identity or stability is uncertain, a thyroid readout becomes hard to trust.
Thyroid peptide studies work best when endpoints match the mechanism under investigation. In immune-mediated models, antibody-focused assays are often central. In endocrine signaling work, hormone profiles matter more.
Common study endpoints include:
That alignment is where good thyroid research separates itself from generic peptide enthusiasm. A peptide intended to modulate autoimmune signaling should be judged very differently from one proposed to influence upstream endocrine signaling.
For researchers who want well-documented materials for laboratory and preclinical workflows, the standard to aim for is simple: transparent batch documentation, consistent analytical testing, and sourcing that supports reproducible study design. Learn more and explore options only when those basics are in place.
If you’re sourcing research peptides for laboratory, analytical, or preclinical work, Peptide Warehouse USA offers US-made compounds with batch-specific documentation, including COAs and supporting quality reports. For teams that value traceability, consistency, and research-use-only compliance, it’s a practical place to explore options.



