No products in the cart.

Search “best peptides for healing” and you’ll mostly find ranked lists, aggressive claims, and very little help with the question that matters. Which compounds have real human evidence, and which ones mainly have preclinical promise?
That distinction changes everything. A peptide can look compelling in cell systems or animal injury models and still remain uncertain for human use, dosing, and long-term safety. If you’re evaluating healing peptides as a researcher, analyst, or informed buyer, popularity isn’t a useful filter. Evidence tier is.
This guide takes a lab-minded view of the field. It focuses on mechanism, research fit, and the difference between biologic plausibility and established human data. You’ll see why BPC-157 gets so much attention, why GHK-Cu occupies a different category, why TB-500 is often discussed in broad recovery contexts, and why the strongest current human-facing support may sit outside the usual injectable peptide conversation.
Which peptide candidates deserve serious attention in healing research, and which ones mainly reflect preclinical enthusiasm amplified by marketing?
Healing peptides sit at the intersection of regenerative biology, translational medicine, and a fast-moving commercial market. That combination creates real scientific interest, but it also creates confusion. Compounds with very different origins, mechanisms, and evidence bases are often discussed as if they belong in the same category.
Some candidates are synthetic research peptides discussed largely because of repeated findings in animal injury models. Others are endogenous human peptides or peptide complexes with better-characterized roles in tissue biology. Those are different starting points, and they should lead to different levels of confidence.

A careful researcher begins by sorting candidates into evidence tiers. At the top are molecules with meaningful human clinical data in a defined indication. Below that are agents supported by human observational or early-phase data. A large share of the healing-peptide discussion sits lower, in mechanistic studies, cell work, and animal models that suggest biological activity without establishing clinical benefit in humans.
That distinction matters because tissue repair is not a single endpoint. Skin closure, tendon remodeling, angiogenesis, scar quality, pain, and return of function are related but separate outcomes. For background on how repair differs across structures, understanding muscles, bones, and joints is a useful reference point. A peptide that looks interesting in one tissue context may not translate cleanly to another.
Working rule: Evaluate healing peptides by target tissue, proposed mechanism, and strength of human evidence.
This approach changes the question in a productive way. Instead of asking for a universal winner, ask whether a given peptide has credible support for the specific repair problem under study, and whether that support comes from cell systems, animal models, or actual human trials.
That is the central filter for this topic. Preclinical promise is common. High-quality human evidence is not.
Tissue repair isn’t one event. It’s a sequence of coordinated cellular programs. Peptides matter because they can influence signaling inside that sequence, sometimes by affecting vascular responses, extracellular matrix behavior, or cell migration patterns.
A useful way to think about them is as signal modulators rather than raw building blocks. They don’t “heal tissue” in a simplistic sense. They may alter how cells behave during repair.
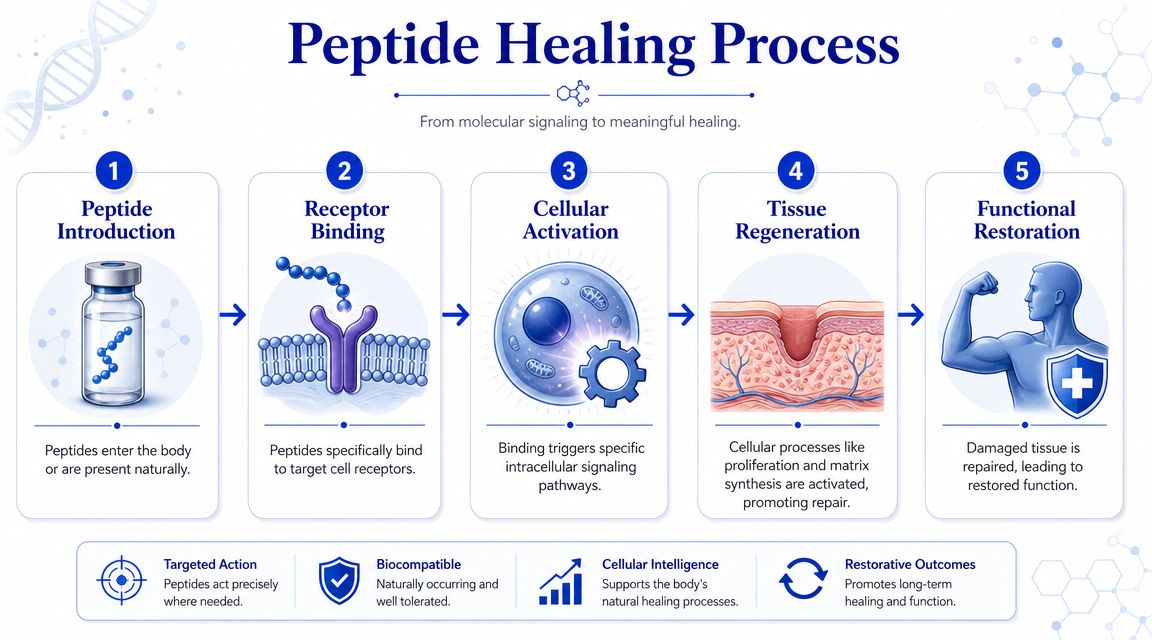
Most tissue repair discussions become clearer when you break healing into broad phases:
For foundational anatomy context, understanding muscles, bones, and joints is a helpful primer because repair behavior differs across tissue types. Muscle, tendon, skin, and ligament don’t respond identically, and that matters when interpreting peptide claims.
Several concepts appear repeatedly in healing-peptide discussions.
The practical implication for a researcher is simple. A peptide should be judged by the biological step it plausibly affects, not by broad “recovery” branding.
This overview is easier to visualize in process form:
Good study design starts by defining the repair event you care about. Matrix deposition, vascularization, re-epithelialization, and functional loading tolerance are not interchangeable outcomes.
That’s why the best peptides for healing can’t be ranked accurately without context. A candidate that’s relevant to skin remodeling may not be the right choice for tendon-focused preclinical work, and a peptide with striking mechanistic interest may still sit on weak human evidence.
Why does BPC-157 dominate healing discussions when the human evidence remains so limited?
The answer is evidence distribution. BPC-157 appears repeatedly in preclinical papers across multiple injury models, so it accumulates visibility faster than compounds supported by narrower but sometimes cleaner datasets. For a researcher, that popularity should trigger closer scrutiny, not faster conclusions.
BPC-157 is usually presented as a synthetic peptide with broad repair relevance in tendon, ligament, muscle, and other soft-tissue contexts. Its appeal comes from recurring findings in animal and in vitro work that suggest effects on repair-associated processes such as vascular signaling, fibroblast activity, and matrix organization. That pattern gives it mechanistic interest across several model systems.
Breadth, however, is not the same as evidentiary strength.
A peptide can look unusually versatile in rodents and still fail the translational tests that matter most. Human efficacy, dosing, tissue-specific pharmacology, adverse-event surveillance, and manufacturing consistency are separate questions. The current BPC-157 literature leaves many of those questions open.
The most defensible conclusion is narrow. BPC-157 remains a preclinical candidate with repeated signal generation, not an established human therapy for tissue repair.
A professional sports medicine review reaches a similar bottom line and argues that enthusiasm for compounds such as BPC-157 has outpaced the available clinical evidence in humans. It points to recurring animal-model findings, then notes the absence of the kind of controlled human trials needed to define safety, dose selection, and reproducible clinical benefit.
That distinction matters because BPC-157 is often cited as if repetition across animal studies settles the therapeutic question. It does not. Repetition can increase confidence that a biological effect is worth studying. It does not establish that the effect is clinically meaningful in humans, or that the risk-benefit profile is acceptable.
A practical evidence-tier framework helps keep the interpretation disciplined:
Interpretive caution: BPC-157 is better understood as a research subject with recurring preclinical promise than as a validated clinical intervention.
That is the non-obvious lesson of BPC-157. In this field, the compounds discussed most often are not always the compounds supported by the strongest human data. Researchers who separate mechanistic plausibility from clinical proof will evaluate healing peptides more accurately and avoid importing marketing logic into evidence review.
How should a researcher interpret a peptide that is discussed widely in repair circles but supported mainly by mechanistic rationale and preclinical work?
TB-500 is better evaluated by starting with identity, not hype. It is generally described as a synthetic peptide fragment associated with thymosin beta-4, whereas thymosin beta-4 itself is the native, full-length peptide involved in actin binding and cell motility. Treating those two as interchangeable weakens the analysis because any inference drawn from the native peptide does not automatically transfer to the fragment.
Thymosin beta-4 has a clearer biological basis in the literature. It has been studied in connection with cell migration, angiogenesis, modulation of inflammatory responses, and organization of the actin cytoskeleton. Those functions make it biologically plausible in tissue-repair research.
TB-500 is usually discussed as a shorter, synthetic analogue intended to capture part of that activity. The problem is not plausibility. The problem is evidence translation. A plausible repair mechanism can justify laboratory interest, but it does not establish clinical benefit, dose selection, product consistency, or safety in humans.
That distinction matters more here than marketing language suggests.
For thymosin beta-4, the literature contains mechanistic studies and animal-model work that support continued investigation in wound and soft tissue repair. For TB-500, public discussion often runs ahead of what is well documented in controlled human studies. The result is an evidence profile that looks stronger at the bench than at the bedside.
A useful way to read this area is by evidence tier:
This ranking changes how a careful reviewer should talk about the peptide. TB-500 belongs in the category of research candidates with translational interest, not established interventions for tissue repair.
The common error is evidence borrowing. Researchers and commentators may cite the biology of thymosin beta-4, then slide into broader claims about TB-500 as if the clinical case were already in place. It is not. Fragment design, formulation, pharmacokinetics, and route of administration can all alter what a peptide does in practice.
So the right question is not whether the mechanism sounds compelling. The right question is whether the specific molecule being discussed has been tested adequately in humans for the outcome being claimed. In the case of TB-500, that standard is still largely unmet.
A disciplined reading therefore leads to a restrained conclusion. Thymosin beta-4 provides a biologically interesting template for repair research. TB-500 remains a preclinical-to-early-translation topic whose reputation currently exceeds its human evidence base.
What should a careful researcher infer when a peptide has plausible endogenous biology, repeated use in skin-focused research, and far less human trial depth than its reputation suggests?
GHK-Cu deserves attention for a narrower reason than many broad “recovery peptide” summaries imply. It is a copper-binding tripeptide discussed primarily in the context of skin biology, extracellular matrix remodeling, and related connective tissue processes. That starting point matters because it changes both the likely endpoints of interest and the standard of evidence required to make a credible claim.
The key point is not that GHK-Cu has a stronger marketing story. It has a more specific biological use case. In research settings, the peptide is typically examined for effects related to collagen production, wound repair signaling, and the quality of tissue remodeling in skin and other connective tissues. Those are different questions from generalized injury recovery, and they should not be collapsed into the same category.
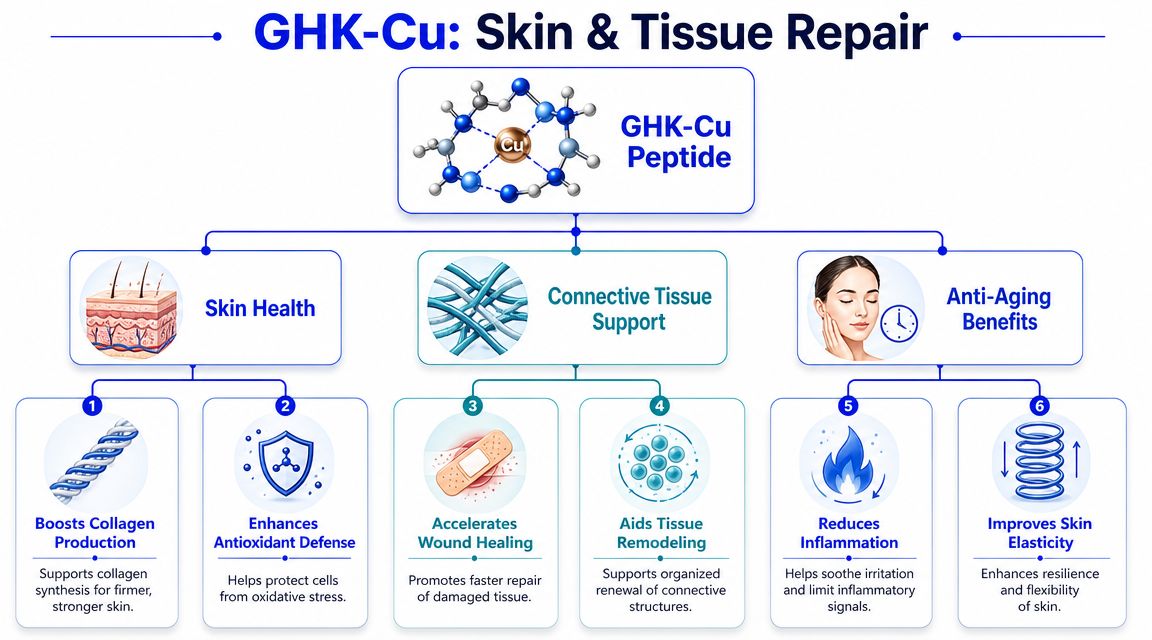
A disciplined reading places GHK-Cu somewhere between mechanistic plausibility and selective translational interest. Preclinical and skin science literature often associates it with matrix regulation, fibroblast-related activity, angiogenic signaling, and tissue appearance outcomes. Those findings justify continued study.
They do not, by themselves, establish broad clinical efficacy in humans across healing applications.
That distinction is easy to miss. Because GHK-Cu is naturally occurring and commonly discussed in dermatologic and cosmetic contexts, readers may assume the human evidence base is deeper than it is. In reality, the case is uneven. The biology is plausible, and the research focus is more tissue-specific than that of many peptides discussed in recovery circles, but high-quality public human trials for clearly defined healing endpoints remain limited.
GHK-Cu is most logically evaluated when the research question centers on:
This matters for study design. If the endpoint is scar quality, dermal remodeling, or connective tissue matrix composition, GHK-Cu may be more relevant than peptides framed around broader repair narratives. If the endpoint is generalized musculoskeletal recovery, the rationale becomes less direct and the evidence case usually weakens.
A useful way to classify GHK-Cu is by evidence tier rather than by popularity. Its mechanistic basis is credible. Its preclinical relevance to skin and connective tissue is stronger than its reputation in generalized healing discussions would suggest. Its human clinical confirmation for many claimed repair outcomes remains sparse.
That makes GHK-Cu a focused research candidate, not a universal answer. The analytical mistake to avoid is treating skin-centered translational promise as proof of established human benefit across all tissue-healing contexts.
How should a researcher compare healing-related peptides when the mechanistic story is often much stronger than the human trial record?
Start by separating popularity from evidence tier. These compounds are often discussed together, but they do not belong in the same evidentiary category. Some have a plausible mechanistic basis and a substantial preclinical literature. Others have narrower but more directly human-relevant support in specific use cases. If those categories are blurred, comparison becomes a marketing exercise rather than a research assessment.
A useful framework begins with the endpoint, then works backward to the peptide. Tissue repair is not one process. Re-epithelialization, collagen remodeling, angiogenic signaling, tendon integration, scar quality, and return of function are related but distinct outcomes. A peptide that looks interesting in a rodent tendon model should not be treated as interchangeable with one studied in skin remodeling or nutritional support for muscle recovery.
Use these questions before ranking any candidate:
Mechanistic fit
Which repair pathway is the peptide plausibly affecting, such as matrix remodeling, cell migration, vascular response, or collagen turnover?
Tissue specificity
Is the literature concentrated in skin, tendon, ligament, muscle, gut-associated injury models, or broad recovery claims with weak tissue definition?
Evidence tier
Is the support based mainly on cell and animal work, early translational interest, or controlled human research tied to a defined healing endpoint?
Endpoint relevance
Are you studying wound closure, biomechanical strength, scar characteristics, imaging changes, pain, or functional recovery? These are not equivalent outcomes.
| Peptide | Primary Mechanism | Primary Research Focus | Evidence Tier |
|---|---|---|---|
| BPC-157 | Commonly discussed in relation to angiogenic signaling, fibroblast activity, and collagen organization | Soft tissue injury models and experimental regeneration settings | Strong preclinical interest, sparse human clinical evidence for defined healing endpoints |
| TB-500 | Commonly discussed in relation to cell migration and actin-associated repair processes | Broad soft tissue repair discussions derived largely from thymosin beta-4 biology | Primarily preclinical rationale, with limited direct human clinical confirmation for healing outcomes |
| GHK-Cu | Copper-peptide activity associated with collagen-related remodeling and wound-relevant signaling | Skin repair, dermal remodeling, and connective tissue biology | More tissue-focused rationale than broad recovery narratives, but human confirmation remains limited for many claimed uses |
| Collagen peptides | Structural substrate support studied alongside rehabilitation or nutrition strategies | Muscle and connective tissue recovery support in selected human contexts | Some human evidence in specific settings, though not interchangeable with regenerative injectable peptide claims |
The main analytical point is easy to miss. If the standard is human evidence for a clearly defined healing outcome, the compounds most discussed in online recovery circles are often not the strongest choices. BPC-157 and TB-500 remain more compelling as preclinical research topics than as clinically established tools. GHK-Cu has a narrower, more coherent rationale in skin and connective tissue work. Collagen peptides sit in a different category altogether, with more human-facing relevance in some contexts but a less dramatic regenerative narrative.
That distinction changes how a serious researcher should read the literature. Preclinical promise answers whether a mechanism is worth studying. Human trials answer whether that mechanism produces a reproducible clinical effect. Those are different questions, and peptide comparisons improve once they are kept separate.
What separates a useful peptide study from a misleading one. Often, it is not the peptide. It is the chain of decisions around evidence tier, material quality, handling, and documentation.
That distinction matters in healing research because the literature is uneven. Several peptides discussed in recovery forums have mechanistic or animal data that justify further study, but far fewer have controlled human evidence for clearly defined healing endpoints. A careful researcher should treat those as different categories from the start. Promising biology is a reason to investigate. It is not proof of clinical effectiveness.

Before procurement or bench work, confirm that the experimental system is defensible on paper as well as in practice:
A recurring problem in peptide work is category confusion. Researchers sometimes compare compounds with sparse human data as if they were established therapeutic tools, then compare suppliers as if branding were a proxy for quality. Neither assumption holds up well.
A better approach is to evaluate two questions separately. First, what level of biological and clinical evidence supports the peptide itself. Second, what level of documentation supports the specific material being used in the experiment. A peptide can be interesting and still poorly validated in humans. A supplier can list an interesting compound and still provide inadequate batch transparency.
| Checkpoint | Why it matters |
|---|---|
| COA availability | Supports batch-level traceability and basic identity review |
| Manufacturing disclosure | Helps assess consistency and sourcing clarity |
| Storage instructions | Lowers avoidable stability and degradation problems |
| Research-use positioning | Keeps procurement aligned with compliance expectations |
One factual example is Peptide Warehouse USA, which states that it supplies research peptides for laboratory, analytical, and preclinical applications and provides lot documentation such as COAs, microbial reports, and endotoxin reports. That kind of record is more useful than broad recovery claims because it addresses reproducibility directly.
The practical conclusion is straightforward. In healing peptide research, good judgment starts with evidence triage. Ask whether a claim is supported by mechanism, animal data, early human observation, or controlled clinical outcomes. Then ask whether the material in hand is documented well enough to generate interpretable results. Supplier transparency is part of study quality, not an afterthought.
If you’re evaluating compounds for laboratory, analytical, or preclinical work, Peptide Warehouse USA is one place to explore options with batch documentation and research-use-only positioning. Learn more about available peptides such as BPC-157, GHK-Cu, and TB-500, review product documentation, and choose materials that fit a rigorous evidence-first workflow.



