No products in the cart.
Individuals searching for Ipamorelin peptide dosage want a neat number. A more pertinent research question is harder: why that number, measured how, delivered by which route, and adjusted based on what response?
That gap matters because ipamorelin sits in a very specific dosing world. The practical conversation is usually about micrograms, not milligrams, and the route, timing, and monitoring plan can change how a protocol is interpreted. For anyone handling this compound in a laboratory, copying a dose range without understanding the logic behind it is weak protocol design.
This guide stays in a research-only context. It explains what ipamorelin is, why common dose ranges cluster where they do, how researchers think about preparation and administration, and how to monitor outcomes instead of treating dosage as a fixed magic number.
What does a dose number mean in ipamorelin research if the protocol around it is poorly defined?
That question matters because dosage is only one variable in a larger experimental system. A stated amount may look precise on paper, yet it says very little by itself. Researchers still need to know what compound was verified, how it was administered, what schedule was used, and which outcomes were tracked.
A useful way to frame ipamorelin peptide dosage is as a set of design decisions rather than a single target value. In lab terms, the dose is one dial on the instrument panel. The other dials include compound identity, administration route, timing pattern, and response monitoring. If one dial is set without the others, interpretation becomes weak.
This is also where newer researchers often get tripped up. They see recurring protocol numbers and assume those numbers are universally correct. In practice, recurring dosage bands usually reflect a mix of published convention, practical handling constraints, and the compound’s proposed signaling behavior. They are starting points for protocol design, not proof that one amount is optimal across settings.
The research-only context needs to stay clear throughout. Ipamorelin is discussed in experimental settings, and dosage decisions should be tied to a defined research question. A protocol aimed at characterizing endocrine response is not identical to one designed to observe recovery-related endpoints over time.
Route of administration adds another layer. Injectable use has the clearer historical footing in peptide research, while newer non-injectable formats generate interest that currently outpaces validation. That gap is easy to miss if a guide only lists common microgram ranges without explaining why route affects absorption, timing, and confidence in the observations.
The goal, then, is not to memorize a few familiar numbers. The goal is to understand why those numbers appear, how to build a protocol around them, and how to judge whether the observed effects can be attributed to the dosing plan rather than to poor experimental control.
Ipamorelin is generally described as a growth-hormone-releasing peptide and a ghrelin mimetic. In plain language, that means it acts like a signal that encourages the body’s growth-hormone system to respond rather than supplying growth hormone directly.
A helpful way to think about ipamorelin is as a key designed for one lock more than many locks. Some compounds trigger broad downstream effects. Ipamorelin is discussed as a more selective signal, which is one reason it remains prominent in peptide research conversations.
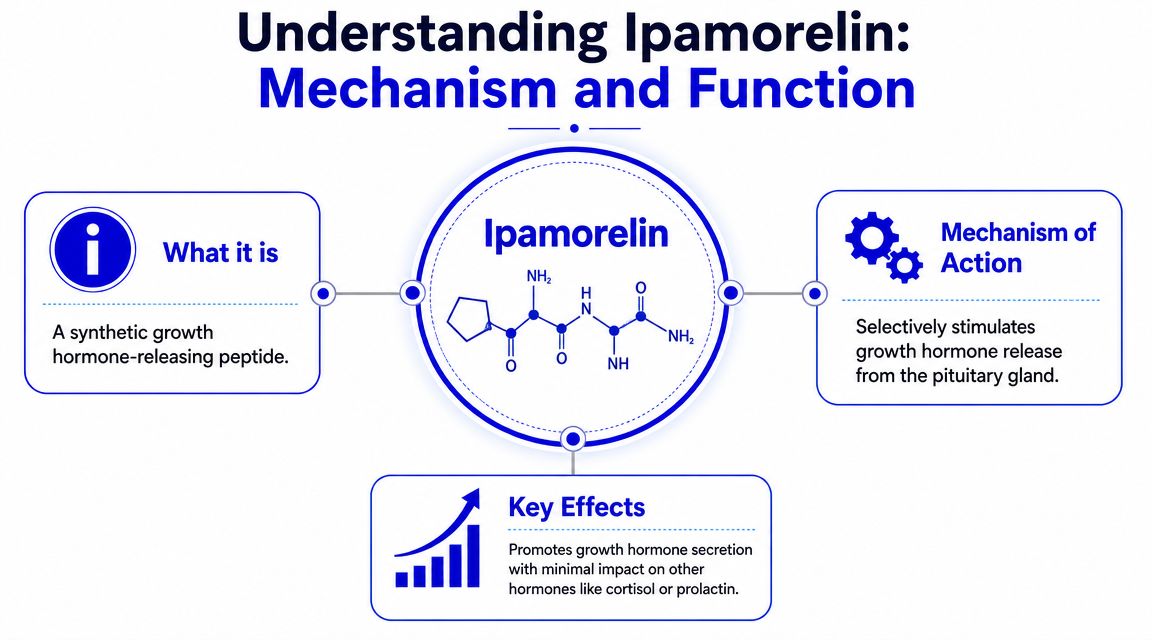
That selectivity is part of why people often compare it favorably with older growth-hormone secretagogues. In research discussions, the attraction isn’t just that it can stimulate growth-hormone release. It’s that the signaling profile is framed as more targeted.
Mechanism and dosage are tightly linked. If a compound is intended to trigger a signaling pulse, researchers usually think about timing and frequency differently than they would for a compound meant to maintain a steady bulk concentration.
That helps explain why common protocol language often centers on bedtime dosing, fasted administration, or split schedules. The idea isn’t random. It’s an attempt to align administration with natural growth-hormone pulsatility.
A junior lab member often gets stuck here and asks a fair question: if the mechanism is selective, why not just keep increasing the amount? The answer is that peptide protocols usually value precision over brute force. With a signaling compound, the shape of exposure can matter as much as the total amount used.
In peptide work, the best protocol often isn’t the highest dose. It’s the clearest test of a defined hypothesis.
Why do ipamorelin protocols get discussed in micrograms instead of broad milligram-style jumps? The short answer is pharmacology. Researchers are working with a signaling peptide, so the question is not only how much is given, but how much is needed to produce a measurable response without obscuring the dose-response pattern.
One early experimental paper helped shape that logic. In a PubMed study on ipamorelin, longitudinal growth rate increased from 42 micrometers/day in the vehicle group to 44, 50, and 52 micrometers/day across treatment groups, with P < 0.0001. That kind of graded response is the reason dosing discussions became narrow and incremental.
The practical lesson is straightforward. If a compound shows stepwise effects across relatively small dose changes, protocol design usually shifts toward tighter control. A researcher does not want dose spacing so wide that one administration is subthreshold and the next is excessive for the question being tested.
A useful lab analogy is receptor titration. If you are adjusting a sensitive assay, you do not change five variables at once and hope the signal becomes clearer. You make controlled, small adjustments so the response curve stays interpretable.
That is the scientific basis for microgram-scale dosing language.
This same study helps explain why titration became normalized in practical protocol discussions, even though many published and market-facing schedules extend beyond what that single paper directly established. The broader idea came first. Researchers observed dose dependence, then built protocols that increase exposure gradually so they can see where response begins, where it improves, and where added dose stops giving useful information.
That distinction matters. Established data support the idea that ipamorelin can show dose-dependent effects in experimental settings. Practical schedules such as starting low, holding for a defined observation period, and increasing in small increments are protocol conventions built around that observation. They are not universal laws.
For a junior lab member, the easiest way to frame titration is this: it separates signal detection from dose escalation. If you start too high, you may confirm that the compound does something, but you learn less about the minimum effective range for your model, the timing of the response, and whether the effect changes meaningfully with added exposure.
A titration design also improves interpretation by keeping one variable in focus:
That is the “why” behind common dosing principles. The point is not to pick a number from a chart. The point is to build a research protocol that can answer a clean question. This becomes even more important when people discuss less-proven delivery methods, because route-related uncertainty can blur the dose-response picture before the experiment even starts.
What does a “standard” ipamorelin dose mean in research. Usually, it means a dose band that appears often enough in protocol discussions to serve as a practical starting reference, not a universally validated rule for every model or route.
That distinction matters. A dose number by itself is only one part of the protocol. The route, timing, observation window, and outcome measures determine whether that number will produce interpretable data.
Research-oriented discussions often cluster around three practical bands for subcutaneous injection. Lower-entry protocols commonly start around 100 to 150 µg daily. A frequently cited middle band is 200 to 300 micrograms per day, often split into two doses. Some higher-exposure protocols discuss totals of up to 400 µg/day.
Those ranges are best understood as working reference points. They show where protocol designers tend to begin, consolidate, or test upper practical limits in routine discussion. They do not establish a single correct dose.
A useful lab analogy is signal calibration. If you are adjusting an instrument, you do not jump straight to the highest setting unless your question specifically requires it. You start in a range that can reveal whether the system responds at all, then increase only if the added exposure helps answer the research question.
Timing choices usually reflect a theory about exposure pattern, not just convenience.
Some protocols use one daily administration, often placed in the evening. Others divide the same total daily amount into morning and bedtime administrations. The scientific rationale is straightforward. If the team wants to examine whether separated exposures produce a different response pattern than a single daily pulse, splitting the dose becomes part of the experimental design rather than a habit copied from forum posts.
Three patterns appear repeatedly:
More injections do not automatically improve a study. They may increase handling burden, reduce consistency, and blur whether a result came from total exposure or from altered timing.
A sharper framing question is this: is the protocol testing a single-pulse exposure model or a distributed daily exposure model?
The table below summarizes dosing patterns commonly discussed in research-oriented material. It is not medical advice and it is not a recommendation for human use.
| Protocol Level | Daily Dosage (mcg) | Administration Frequency | Example Cycle Length |
|---|---|---|---|
| Entry range | 100 to 150 | Once daily | 8 to 12 weeks |
| Foundational range | 200 to 300 | Often split into two doses | 8 to 12 weeks |
| Advanced discussion range | Up to 400 | Often divided across the day | Up to 16 weeks |
The table is useful only if you read it as a map of protocol intent.
The entry range is often the cleanest choice when the objective is baseline sensitivity testing. The foundational range appears often because it sits in the middle of current protocol discussions, not because it is mandatory. The advanced discussion range increases exposure and scheduling complexity, which may be appropriate for some designs but can weaken a narrow, mechanism-focused study if too many variables shift at once.
Route also needs to stay in view. These dosage bands are usually discussed in the context of injectable administration. If a researcher is considering an emerging delivery method with less established absorption characteristics, the same nominal microgram amount may not represent the same real exposure. That is one reason route selection should be locked before dose comparisons begin.
If you’re comparing procurement options for a protocol that includes ipamorelin-containing products, some researchers review formulations such as the CJC-1295 (No-DAC) + Ipamorelin blend from Peptide Warehouse USA alongside standalone materials, then calculate the planned dose from the exact vial concentration and the specific research design.
Handling quality matters as much as protocol logic. A precise dose written on paper means little if the peptide is reconstituted carelessly or stored poorly.
A visual workflow helps keep the process consistent.
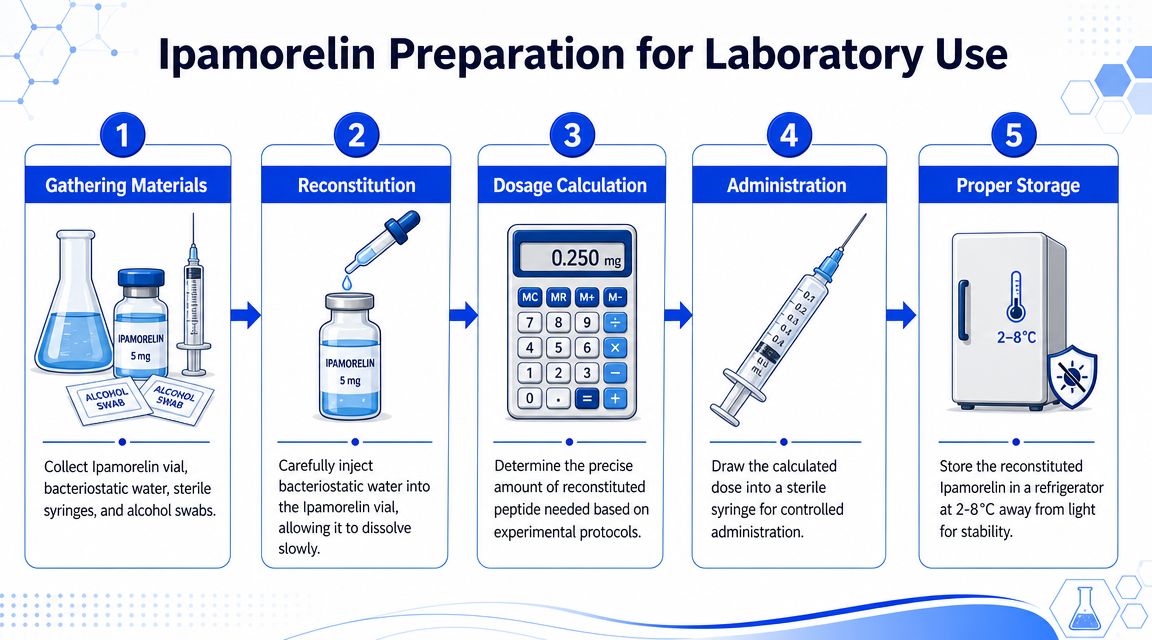
In routine lab handling, researchers typically begin with a lyophilized peptide and reconstitute it using an appropriate sterile diluent. The point of reconstitution isn’t just dissolving the powder. It’s creating a solution concentration that allows accurate measurement for the planned protocol.
A clean workflow usually includes:
Later in the same workflow, some teams like a quick visual reference for administration and storage basics.
Subcutaneous injection remains the most established and studied route for ipamorelin, while some practitioners are exploring oral or nasal forms. At the same time, the market narrative around those alternatives is expanding faster than the evidence for efficacy and bioavailability, as noted in this clinic discussion of ipamorelin peptide therapy.
That’s an important correction to common online messaging. Novel delivery formats may sound easier, but convenience doesn’t equal validation.
For a research-minded reader, the route question should be framed like this:
The biggest weakness in most dosage content is that it stops at “how much.” A stronger protocol starts with “what counts as a response?”

Many dosage guides don’t explain how to measure response. Practical guidance increasingly emphasizes that effective protocol design is iterative, meaning researchers start conservatively, monitor specific outcomes, and adjust based on collected data and qualified oversight rather than chasing a universal microgram target.
That idea changes everything. Instead of asking, “What is the right dose?” ask:
A protocol without those answers turns dosage into guesswork.
Practical rule: Change one major variable at a time. If you alter dose, timing, and route together, you won’t know what caused the result.
The specific monitoring plan depends on the model and study aim, so it should be adapted. Still, the thinking process is fairly universal.
A useful monitoring sheet often includes:
Readers often want a list of exact biomarkers. In many real-world protocol discussions, that level of standardization isn’t there. That’s part of the content gap. The evidence base is heavily protocol-driven, so monitoring has to be built around the specific research question rather than copied from a one-size-fits-all template.
A cautious summary is the right summary here. Ipamorelin is often discussed as having a relatively selective signaling profile compared with older compounds in the same category, which is one reason it stays relevant in peptide research.
The cleanest established point is not that it’s “safe” in a broad consumer sense. It is that researchers often view it through the lens of targeted growth-hormone release and microgram-scale precision, not broad systemic dosing. That framing supports careful, controlled protocol design.
Many articles often overreach. If a source set doesn’t provide quantified adverse-event data, the responsible move is to stay qualitative.
So the practical safety discussion should focus on process:
The most responsible conclusion is simple. Ipamorelin should be treated as a research compound requiring controlled handling, precise dosing logic, and conservative interpretation. It should not be discussed casually as if route, timing, and response measurement are interchangeable.
What should a researcher carry forward after reviewing ipamorelin peptide dosage. A dosing range is only the starting point. The more useful endpoint is a protocol that connects mechanism, route, preparation, timing, and outcome tracking into one interpretable system.
That distinction matters. Two studies can use similar microgram ranges and still produce findings with very different value if one controls reconstitution, administration timing, and observation windows while the other changes multiple variables at once. In practice, dosage only means something when it is tied to a clear question and a repeatable method.
Ipamorelin works like a signaling tool, not a blunt input. That is why the strongest dosage discussions focus on rationale, not just common numbers passed between labs. The established research logic still centers on injectable administration, especially subcutaneous use, because that route has the clearest procedural footing in the literature and in routine laboratory handling. Less-proven delivery methods may be interesting to examine, but they should be treated as separate experimental questions rather than interchangeable substitutes.
A careful protocol also needs a plan for reading results. Before selecting a dose, define what will count as a meaningful observation, how often it will be recorded, and which confounding variables will be held steady. That approach makes interpretation cleaner and reduces the risk of mistaking handling error, route changes, or protocol drift for a compound-specific effect.
The final point is simple. Ipamorelin belongs in research, laboratory, and analytical settings only.
For researchers evaluating suppliers during procurement review, Peptide Warehouse USA offers USA-made research peptides and related compounds for laboratory and analytical use only, along with batch documentation and product information.



