No products in the cart.

You may be comparing notes from a protocol draft, a vendor catalog, and a handful of peptide discussions that seem to blur together. That’s usually where the confusion starts. Tesamorelin and Ipamorelin are often grouped as if they do the same job, but they don’t. They engage different signaling routes, and that difference is the whole reason the Tesamorelin and Ipamorelin blend attracts attention in laboratory settings.
For researchers studying metabolic regulation, pituitary signaling, or growth hormone pulse behavior, this blend is best understood as a mechanistic pairing rather than a proven combination therapy. One component has a formal clinical history. The other is valued for receptor selectivity in research. The useful question isn’t “Are they similar?” It’s “What distinct signal does each peptide contribute, and why might those signals be worth testing together under controlled conditions?”
The most productive way to evaluate this blend is to separate hype from mechanism. In a research context, these peptides are interesting because they don’t duplicate each other. Tesamorelin acts through the GHRH receptor axis, while Ipamorelin is described as a selective ghrelin-mimicking growth hormone secretagogue.
That distinction matters in experimental design. If a lab wants to observe what happens when two upstream growth hormone signals are engaged at the same time, this pairing offers a clear conceptual model. It’s less about stacking similar compounds and more about testing whether different pituitary inputs produce a broader or sharper secretory response.
A colleague new to the topic often gets stuck on one point: if Tesamorelin already has human data, why add Ipamorelin at all? The reason is mechanistic, not regulatory. Tesamorelin brings the stronger evidence base. Ipamorelin brings a selective signal that may help isolate ghrelin-pathway contribution in controlled studies.
The blend makes the most sense when the research question is about signaling architecture, pulse behavior, or pathway interaction, not when someone treats it like an established finished therapy.
A useful way to frame the blend is this:
Everything after that depends on rigor. These materials are for research use only, and any interpretation should stay inside laboratory, analytical, or preclinical boundaries.

A lab studying this blend usually starts with one practical question: which component provides the firmer interpretive baseline? For most research designs, that baseline is Tesamorelin.
Tesamorelin is a growth hormone-releasing hormone analog. It acts at the GHRH receptor level, so it probes the hypothalamic-pituitary growth hormone axis through the receptor class normally associated with endogenous GHRH signaling. That matters because it gives researchers a defined upstream input. In experimental terms, Tesamorelin helps answer, “What happens when the pituitary receives a GHRH-like cue?” rather than “What happens after growth hormone is already present?”
Its translational relevance is different from Ipamorelin’s. Tesamorelin has an FDA-approved clinical history in the United States for reducing excess abdominal fat in HIV-associated lipodystrophy. Ipamorelin does not carry that same level of human regulatory validation. For a research scientist, that distinction shapes how each peptide should be interpreted in a blend model.
The value of Tesamorelin is not only that it stimulates growth hormone release. Many compounds are discussed in those broad terms. Tesamorelin is more useful because its receptor target and human study history give the blend a clearer mechanistic and evidentiary center.
A simple way to frame it is to compare signaling routes. Tesamorelin addresses the GHRH-R side of pituitary stimulation. Ipamorelin, discussed separately, is generally studied as a ghrelin-mimetic secretagogue. Those are related inputs, but they are not interchangeable. Using Tesamorelin in a blend lets researchers test one side of that dual-input hypothesis with a peptide that already has established human clinical exposure.
That makes Tesamorelin the anchor for study design, endpoint selection, and interpretation. If a preclinical model shows changes in GH-associated or IGF-1-associated biology after exposure to the blend, Tesamorelin provides the better-characterized half of the signaling pair.
| Research question | Why Tesamorelin fits |
|---|---|
| Pituitary GHRH-pathway stimulation | It models signaling through the GHRH receptor axis |
| Endocrine pulse architecture | It provides a defined upstream hypothalamic-style input |
| Translational comparison work | It contributes the stronger human evidence base in the pair |
One point often causes confusion. Tesamorelin’s clinical history does not validate the blend as a finished intervention. It only means one component has been studied in humans far more extensively than the other.
Research-use interpretation: Tesamorelin should be treated as the clinically characterized component of the pair, useful for anchoring mechanistic hypotheses about GHRH-receptor signaling in laboratory and preclinical settings only.
That distinction protects the logic of the experiment. Tesamorelin contributes the better-established GHRH-pathway signal. Ipamorelin contributes a separate secretagogue pathway that may modify, amplify, or reshape that signal in preclinical systems. The blend hypothesis depends on those pathways being different enough to study together, not on treating both peptides as if they carry the same level of clinical evidence.
A common mistake is to treat Ipamorelin as just another GH booster. In laboratory terms, that framing is too vague to support good experimental design. Ipamorelin is more usefully described as a growth hormone secretagogue studied for ghrelin-like activity, which places it on a different upstream control route than Tesamorelin.
That distinction matters because the question is not only whether GH output changes. The question is which receptor system was perturbed, how selectively it was perturbed, and whether the resulting endocrine pattern is easier to interpret than with older secretagogues.
Ipamorelin is often discussed as a more selective member of the GHRP category. The practical reason is straightforward. In preclinical and research discussions, it is commonly presented as favoring GH release with less spillover into other pituitary hormone signals than less selective secretagogues.
For study design, that narrower signal can be useful.
If a compound perturbs several endocrine axes at once, attribution becomes difficult. A rise in a downstream marker may reflect mixed upstream inputs rather than the pathway under study. Ipamorelin is attractive in mechanistic work because it is often chosen to add a ghrelin-mimetic input without deliberately introducing as much background endocrine noise as broader secretagogues might.
A laboratory analogy helps here. Tesamorelin works like one control line entering the somatotroph through the GHRH receptor. Ipamorelin is investigated as a second control line that resembles ghrelin receptor signaling. If the second line is relatively selective, the combined experiment is easier to interpret because the investigator is varying two defined inputs rather than adding a poorly bounded stimulus.
Its role in the pair is conceptual before it is translational. Tesamorelin supplies the better characterized GHRH-receptor stimulus. Ipamorelin contributes the ghrelin-mimetic side of the model. That division of labor is the reason researchers remain interested in the combination.
Three points keep the logic clear:
A narrower endocrine signal can improve interpretability, but it does not convert a research peptide into a clinically established intervention.
One regulatory distinction should stay explicit throughout the article. Ipamorelin remains a research compound and does not share Tesamorelin’s FDA-approved status. In laboratory writing, that means hypotheses about the blend should separate established evidence for Tesamorelin from exploratory, preclinical reasoning about Ipamorelin.
A common laboratory question is straightforward. If one peptide stimulates the growth hormone axis through the GHRH receptor and another engages the ghrelin-responsive secretagogue pathway, does concurrent exposure produce a different signal pattern than either input alone?
That question is the scientific basis for combining tesamorelin and ipamorelin in research settings.
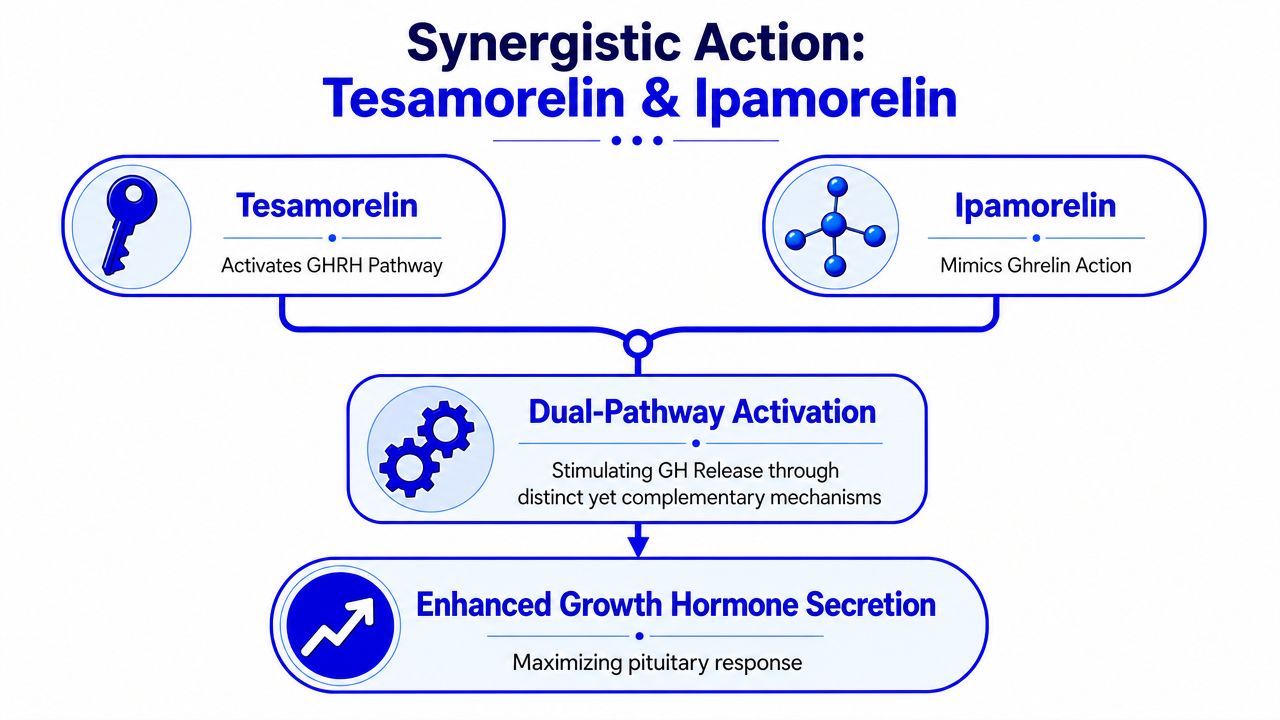
Tesamorelin and ipamorelin are grouped together because they are proposed to influence the same endocrine axis through different upstream receptors. Tesamorelin is a GHRH analog, so its primary mechanistic role in this model is GHRH receptor activation. Ipamorelin is studied as a selective growth hormone secretagogue that mimics ghrelin-like signaling, typically discussed in relation to the ghrelin receptor pathway.
The distinction matters. A two-agent design is only informative if each component contributes a separate experimental input. In this blend, tesamorelin represents the GHRH-R side of the system. Ipamorelin represents the ghrelin-mimetic side. Researchers are therefore not asking whether the same signal can be repeated twice. They are asking whether parallel receptor engagement changes pulse dynamics, downstream biomarkers, or tissue responses.
A useful comparison is a control system with two upstream switches feeding one output node. One switch regulates the GHRH channel. The other regulates the ghrelin-linked secretagogue channel. If both switches are active during the same interval, the output may change in amplitude, timing, or pattern.
This visual helps clarify the model:
In a laboratory context, synergy should be defined narrowly. It refers to the hypothesis that combined stimulation of GHRH-R and ghrelin-responsive signaling produces an effect that differs meaningfully from single-pathway stimulation under matched conditions.
That does not establish clinical benefit.
The strongest support in this pairing belongs to tesamorelin, which has an FDA-approved clinical history in a specific indication. Ipamorelin does not share that status and remains a research peptide. For that reason, any discussion of the blend has to keep two evidence tiers separate. Tesamorelin contributes a clinically characterized reference point. Ipamorelin contributes a preclinical mechanistic variable.
That separation prevents a common error. Mechanistic plausibility is not the same as validated therapeutic performance.
The proposed complementarity comes from receptor biology. GHRH-receptor activation helps drive somatotroph signaling in one way. Ghrelin-mimetic stimulation is hypothesized to modulate the same axis through a different receptor system. When both inputs are present in the same experiment, investigators can examine whether the combined condition changes GH secretory behavior relative to tesamorelin alone, ipamorelin alone, or control exposure.
The practical readout is rarely just “more GH.” In a well-designed preclinical study, the more informative question is whether the pattern changes. Researchers may look for differences in pulse amplitude, pulse frequency, timing of release, downstream IGF-1 directionality, or tissue-specific metabolic signals. That is where the blend becomes mechanistically interesting.
A simple stepwise model looks like this:
The value of the blend is strongest in controlled research use only settings, where pathway interaction can be isolated, measured, and interpreted with appropriate controls. Outside that context, the evidence base becomes uneven quickly, because one peptide has an approved clinical track record and the other remains preclinical.

A useful preclinical model starts with a narrow question. If one investigator wants to measure how GHRH receptor signaling shapes downstream metabolic readouts, and another wants to test whether ghrelin-mimetic input changes that pattern, the tesamorelin and ipamorelin blend gives them a way to examine both inputs within the same experimental frame. The scientific value comes from separating what is already grounded in tesamorelin data from what remains hypothetical for the combination and for ipamorelin itself.
That distinction matters. Tesamorelin has an FDA-approved clinical history in a specific indication, which gives researchers a firmer reference point for GH-axis and visceral adiposity questions. Ipamorelin does not carry that same clinical status. In laboratory settings, its role is better understood as a selective growth hormone secretagogue used to probe mechanism, not as a clinically validated counterpart to tesamorelin.
One of the clearest applications is metabolic modeling that asks whether dual-pathway stimulation changes where, when, or how a response appears. Tesamorelin is often the anchor peptide for this type of work because its biology has been studied more extensively in relation to visceral fat and endocrine signaling. Adding ipamorelin lets investigators test whether ghrelin-receptor pathway activation shifts the response pattern rather than an increase limited to a single endpoint.
A practical analogy is two switches feeding the same circuit through different lines. The output may rise, but the more interesting result is often a change in timing, signal shape, or tissue preference.
Potential study directions include:
Those questions are appropriate for research use only because they test mechanism under controlled conditions. They do not justify treating the blend as if it carries the same level of human evidence as tesamorelin by itself.
A second application area is GH secretory dynamics. Here, the blend is useful because the readout is not limited to absolute hormone output. Researchers can compare pulse amplitude, pulse timing, exposure sequencing, receptor-specific antagonism, and downstream IGF-1 directionality to see whether concurrent GHRH-R and ghrelin-mimetic stimulation produces an additive effect or a true synergistic one.
| Model focus | Why the blend is useful |
|---|---|
| Pulse amplitude studies | Dual upstream inputs can be tested for changes in secretory magnitude and shape |
| Timing studies | Sequential versus simultaneous exposure can clarify whether order affects response |
| Receptor contribution work | Experimental controls can help separate GHRH-receptor and ghrelin-pathway effects |
Tissue-response and aging-related models are also common, but they require tighter language and tighter controls. Researchers may use the blend to examine recovery-associated biomarkers, protein turnover signals, or cell-level repair pathways in model systems. The defensible claim is that the blend can help test a hypothesis about pathway interaction. The defensible claim is not that it is an approved intervention for aging or performance.
Handling discipline also affects interpretability in these studies, especially where repeated dosing, reconstitution, or exposure timing can influence assay outcomes. Labs building protocols around peptide materials should align those workflows with established principles of laboratory hazardous drug safety, batch documentation, and exposure control.
For procurement and study planning, some laboratories may choose a pre-formulated paired product rather than sourcing each peptide separately. Peptide Warehouse USA offers a Tesamorelin and Ipamorelin blend presented for laboratory, analytical, and preclinical use rather than human consumption. In a research context, that format can reduce sourcing variability when the protocol specifically calls for fixed-ratio evaluation of both compounds.
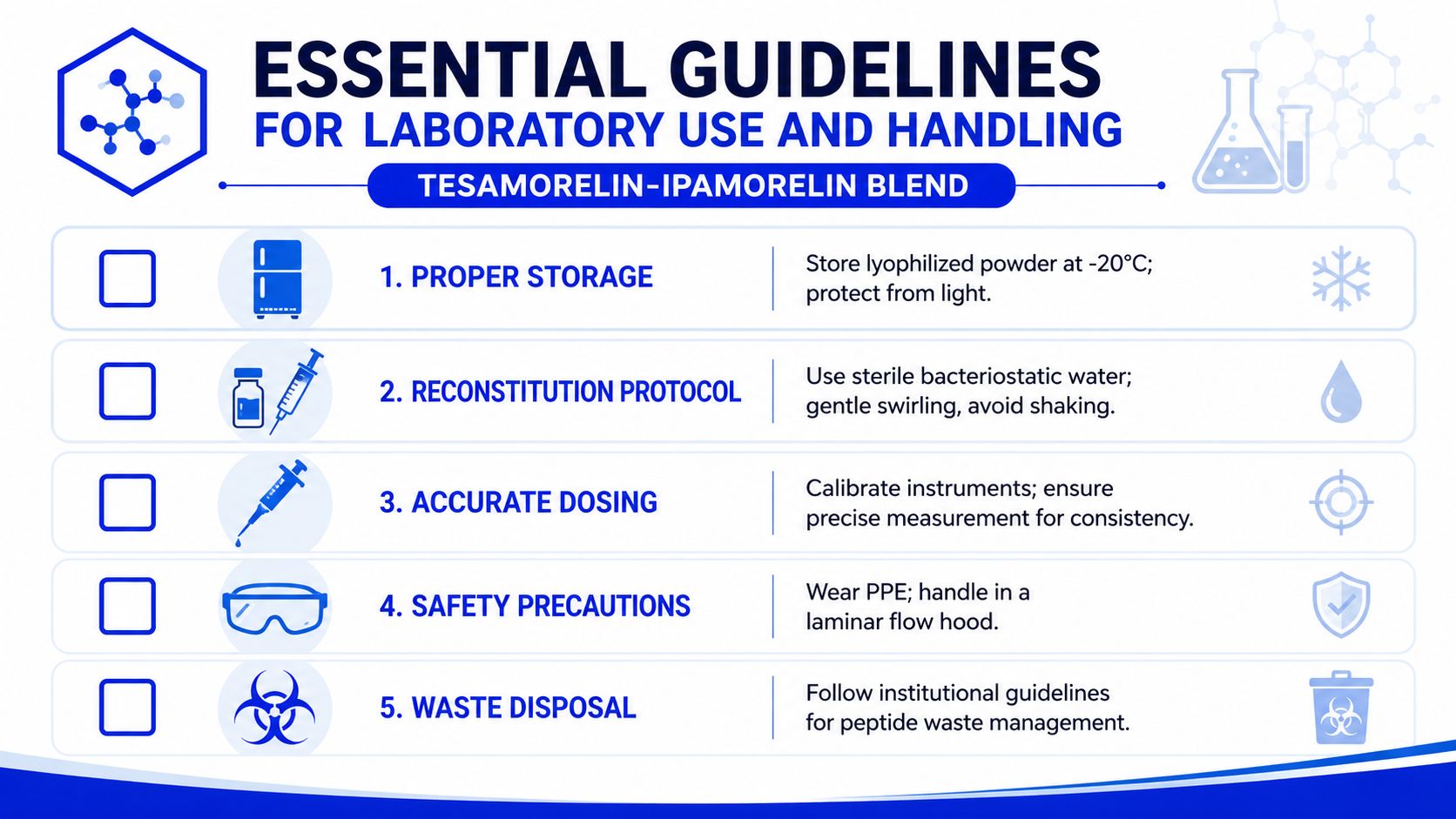
A peptide blend only answers a scientific question if the material stays stable, traceable, and consistently handled. Most experimental problems blamed on “weak compound performance” start much earlier, usually at storage, reconstitution, or measurement.
Researchers should establish a documented chain from receipt to final use. That means logging batch identity, reviewing the accompanying paperwork, assigning storage conditions, and limiting unnecessary freeze-thaw exposure.
A disciplined workflow usually includes:
If your team works with compounds that require heightened handling awareness, it’s worth reviewing broader guidance on laboratory hazardous drug safety. The article is useful because it reinforces practical controls such as PPE, engineering controls, and waste discipline that improve peptide-handling reliability too.
Lab note: Consistency beats speed. A slower, documented reconstitution process is better than a fast one that introduces concentration drift.
Labs commonly reconstitute lyophilized peptides using sterile bacteriostatic water, but the exact procedure should follow supplier instructions and internal protocol requirements. The goal is simple: create a solution with a known concentration while minimizing degradation risk and physical stress to the peptide.
A sound reconstitution workflow looks like this:
The hardest part for many new researchers isn’t the physical handling. It’s resisting informal shortcuts. If one analyst reconstitutes by volume estimate and another uses calibrated measurement, the study has already introduced avoidable variability. The blend may be mechanistically interesting, but only disciplined handling makes the data interpretable.
A common failure point appears before any assay begins. A lab receives a vial labeled as a tesamorelin and ipamorelin blend, the label looks clean, and the peptide enters a study pipeline without anyone confirming what, exactly, was verified. At that point, the scientific question has already shifted from receptor biology to batch uncertainty.
For this blend, quality control has two jobs. First, it establishes whether the material matches the stated identity and purity specifications. Second, it protects interpretation of a dual-mechanism study, where one component has a defined regulatory record and the other remains preclinical. If either part is poorly documented, it becomes difficult to tell whether an observed effect reflects GHRH receptor signaling, ghrelin-receptor agonism, formulation variability, or contamination.
Procurement review should therefore focus on traceability, not appearance. Researchers should confirm a batch-specific Certificate of Analysis, lot number, identity testing, and purity data before the material is accepted into inventory. For laboratories studying cell systems, tissue models, or animal models with tighter contamination controls, microbial and endotoxin documentation can also matter because those variables can distort downstream readouts.
The logic is the same as calibrating an instrument before collecting data. If the starting material is uncertain, mechanistic conclusions become weaker even when the experimental design is otherwise careful.
Regulatory language should be explicit. Tesamorelin has an FDA-approved reference point in a specific clinical context. The prescribing information for EGRIFTA SV describes tesamorelin as a synthetic 44-amino-acid growth hormone-releasing factor analog with a hexenoyl group, supplied as 2 mg lyophilized powder for subcutaneous use, and notes its effect on growth hormone secretion with subsequent increases in IGF-1 and IGFBP-3, as detailed in the FDA prescribing information for EGRIFTA SV.
That approved status does not extend to ipamorelin. It does not extend to a tesamorelin and ipamorelin blend, either. In research terms, that distinction matters because the blend is often discussed for its hypothesized synergy. Tesamorelin is used to probe the GHRH-R pathway. Ipamorelin is used to probe selective ghrelin-mimetic signaling. Combining them may help researchers examine whether two upstream inputs produce a stronger or differently timed GH-axis response in preclinical systems. But a mechanistic hypothesis is not a regulatory approval.
The disclaimer should therefore state the use case plainly. This blend is for research use only, limited to controlled laboratory, analytical, and preclinical settings. It is not an approved combination therapy, not a dietary supplement, and not intended for human consumption.
Clear disclaimers do more than reduce compliance risk. They keep the scientific framing honest. Tesamorelin can be discussed with reference to approved labeling in its authorized context. Ipamorelin should be described as a research peptide with preclinical relevance, not as an approved therapeutic agent. That separation helps prevent overstatement and keeps experimental claims aligned with the actual evidence base.
The value of this blend comes from division of labor. Tesamorelin supplies the stronger clinical and mechanistic anchor. Ipamorelin supplies a selective ghrelin-mimetic input that makes dual-pathway testing scientifically interesting. Together, they form a useful research model for labs studying GH-axis signaling, metabolic regulation, and related preclinical endpoints.
The key is discipline. Use verified material, document handling carefully, and keep every claim inside the limits of research evidence. If you’re evaluating options for upcoming studies, learn more about high-purity research materials and explore options that fit a controlled laboratory workflow.
If you’re sourcing materials for peptide studies, Peptide Warehouse USA offers research peptides and related compounds for laboratory, analytical, and preclinical applications, with batch documentation and compliance-focused labeling that can support a more traceable procurement process.



