No products in the cart.

For a clear answer on LL-37 peptide dosage, you’ve already run into the main problem. Most compounds let you ask, “What dose works?” LL-37 forces a harder question: “What concentration works in which model, by which route, and under what local conditions?”
That difference matters. LL-37 is a human host-defense peptide with broad research interest, but its behavior is highly context-sensitive. In one setting, lower concentrations may support the effect a lab wants to study. In another, pushing the concentration higher may reduce benefit or even create unwanted toxicity. That’s why simple dosing charts often mislead more than they help.
Researchers usually get confused in three places. First, they mix in vitro concentration with in vivo dose. Second, they compare topical human data with systemic animal work as if they were interchangeable. Third, they assume a larger amount should produce a stronger response. The published literature doesn’t support that shortcut.
LL-37 sits in a category that researchers often underestimate. It isn’t just a peptide with one narrow effect. It’s part of the body’s innate immune system, which means it behaves more like a rapid-response signal and barrier-defense molecule than a simple on-off reagent.
A useful analogy is a first-responder team. The same responders may secure a scene, direct traffic, call for backup, and help with cleanup. LL-37 has that same multi-role character in research. People study it because it has been associated with antimicrobial activity, chemotaxis, immune signaling, and tissue-repair processes.
That complexity is exactly why LL-37 peptide dosage is hard to standardize. Dose isn’t just about how much material goes into a vial, syringe, dish, or topical base. It’s about where the peptide ends up, how concentrated it becomes at the local site, how long it remains there, and what cells or tissues it encounters.
Practical rule: With LL-37, the most useful question isn’t “What’s the universal dose?” It’s “What exposure range matches my model without crossing into the wrong biological effect?”
LL-37 is the only known human cathelicidin peptide, which is one reason it gets so much attention in peptide research. It’s part of the host-defense toolkit that the body deploys at barrier surfaces and sites of injury or microbial challenge.
Researchers don’t study LL-37 for only one reason. They study it because it appears across several biological themes at once:
That combination makes LL-37 scientifically interesting, but it also makes interpretation tricky. A peptide with one dominant effect is easier to dose than a peptide that can shift behavior depending on concentration and environment.
A common mistake is assuming LL-37 should have one preferred research dose across all applications. The literature suggests the opposite. Published work shows dose-dependent, opposing effects, where low nanomolar to micromolar levels can be anti-biofilm, chemotactic, or antimicrobial, while concentrations above about 10 µM may become cytotoxic, as described in the review discussing LL-37 concentration-dependent behavior.
That’s the core idea many simplified guides miss. LL-37 isn’t just “stronger at higher dose.” It can change categories of effect as concentration rises.
The same molecule can look helpful in one assay and harmful in another, simply because the local concentration moved into a different biological window.
That’s why smart experimental design starts with the research question. Are you probing microbial interaction, chemotaxis, epithelial response, or topical tissue behavior? Each question may call for a different exposure range and a different formulation logic.
The hardest part of LL-37 work is accepting that there may never be one tidy universal dose. That’s not a weakness in the literature. It’s a reflection of the peptide’s biology.

Many researchers approach peptides as if dose-response should rise smoothly. LL-37 doesn’t fit that mental model well. In practical terms, a low concentration may support one kind of measured response, while a higher concentration may flatten the effect, reverse it, or introduce toxicity.
That pattern shows up clearly in human topical data. In a randomized chronic leg-ulcer study, 0.5 mg/mL and 1.6 mg/mL LL-37 improved healing versus placebo, with healing-rate constants about sixfold and threefold higher than placebo, and mean ulcer area reductions of 68% and 50%, while the 3.2 mg/mL group did not outperform placebo. The study reported no local or systemic safety concerns in that setting, and the lower topical concentrations had the strongest support in that human dataset, as reported in the PubMed summary of the chronic leg-ulcer trial.
That result matters because it breaks the “more is better” assumption. If a higher concentration doesn’t improve the outcome, it suggests a therapeutic window rather than an open-ended dose ladder.
Another reason LL-37 dosage looks inconsistent is that researchers often compare values that don’t belong in the same bucket.
Common examples include:
A vial amount tells you almost nothing by itself. Biology responds to exposure concentration at the target site, not to how much dry peptide you own.
Here’s the practical distinction:
That’s why one lab may report a useful concentration in vitro, while another publishes a weight-based animal dose, and neither number can be copied directly into the other experiment.
For bench work, LL-37 should be framed as a concentration problem, not a “dose” problem in the casual sense. In vitro studies usually report exposure in nM, µM, or µg/mL, because those units describe what cultured cells or microbes are exposed to.
The literature summary provided for this topic supports a broad qualitative rule. LL-37 can show anti-biofilm, chemotactic, or antimicrobial activity at lower nanomolar to micromolar levels, while higher concentrations may move toward cytotoxicity. That means your first draft experiment shouldn’t jump straight to the top of the range.
A practical way to organize planning is with a simple screening table.
| Research Application | Typical Concentration (µM) | Typical Concentration (µg/mL) |
|---|---|---|
| Exploratory low-range signaling work | low nanomolar to low micromolar | convert from target molarity based on peptide molecular weight |
| Anti-biofilm or chemotactic screening | low nanomolar to micromolar | convert from target molarity based on peptide molecular weight |
| Antimicrobial screening | micromolar range may be explored | convert from target molarity based on peptide molecular weight |
| Upper-range stress testing | approach with caution because above about 10 µM may become cytotoxic | convert from target molarity based on peptide molecular weight |
The table stays partly qualitative on purpose. The verified literature supports the concentration bands concept, but it does not provide a validated universal in vitro chart for each assay type. That restraint is part of good research practice.
Most confusion comes from unit conversion, not from biology.
Use this sequence:
For example, if you want to compare a lower exploratory condition against a higher one, you’d create a stock, then add calculated volumes into separate wells to reach the final desired molarity. The key point isn’t the arithmetic alone. It’s that every condition should be calculated from the final exposure in the well.
If the calculation starts from “I have a vial with X milligrams,” you’re starting in the wrong place. Start from the concentration you want cells to experience.
Useful bench habits include:
Once LL-37 moves from a dish into an animal model, the language changes. Concentration still matters, but researchers usually report mg/kg or mg/kg/day, and route starts to dominate interpretation.
A topical dose, a subcutaneous dose, and an intraperitoneal dose don’t represent the same biological situation. They create different local concentrations, different distribution patterns, and different exposure durations.
The verified background for this article highlights that the clinical data are available primarily for topical application, with human wound studies using 0.5–1.6 mg/mL, while preclinical experiments used a much wider range, including systemic doses up to 1 mg/kg/day in rats and 5 mg/kg/day in mice, as summarized in the LL-37 dosage review page describing human topical and animal systemic ranges.
That contrast tells you two things:
Weight-based calculation is straightforward once the target dose is defined for the model.
Suppose a protocol uses 1 mg/kg/day in a rat model. For a 250-gram rat, first convert body weight to kilograms:
Then multiply:
If your reconstituted solution contains a known concentration, you then calculate the administration volume needed to deliver 0.25 mg. The exact injection volume depends entirely on the concentration you prepared.
Many errors occur at this point. Labs often do the first multiplication correctly, then prepare a stock that makes the administration volume awkward or inaccurate. Good planning works backward from a practical delivery volume.
A clean workflow looks like this:
A reported mg/kg value isn’t a universal protocol. It’s one component of a full design that includes route, formulation, timing, and endpoint selection.
Another important point is duration. The broader LL-37 literature remains less standardized outside topical use. The available summary notes topical treatment durations of up to 4 weeks and oral-capsule exposure for up to 7 days, reinforcing that LL-37 development has centered on relatively short-course experimental protocols rather than an established systemic standard. That context comes from the same earlier linked review source.
Even a good protocol can fail if the peptide is handled poorly. LL-37 is typically supplied as a lyophilized powder, which is the most practical format for preserving stability before use.
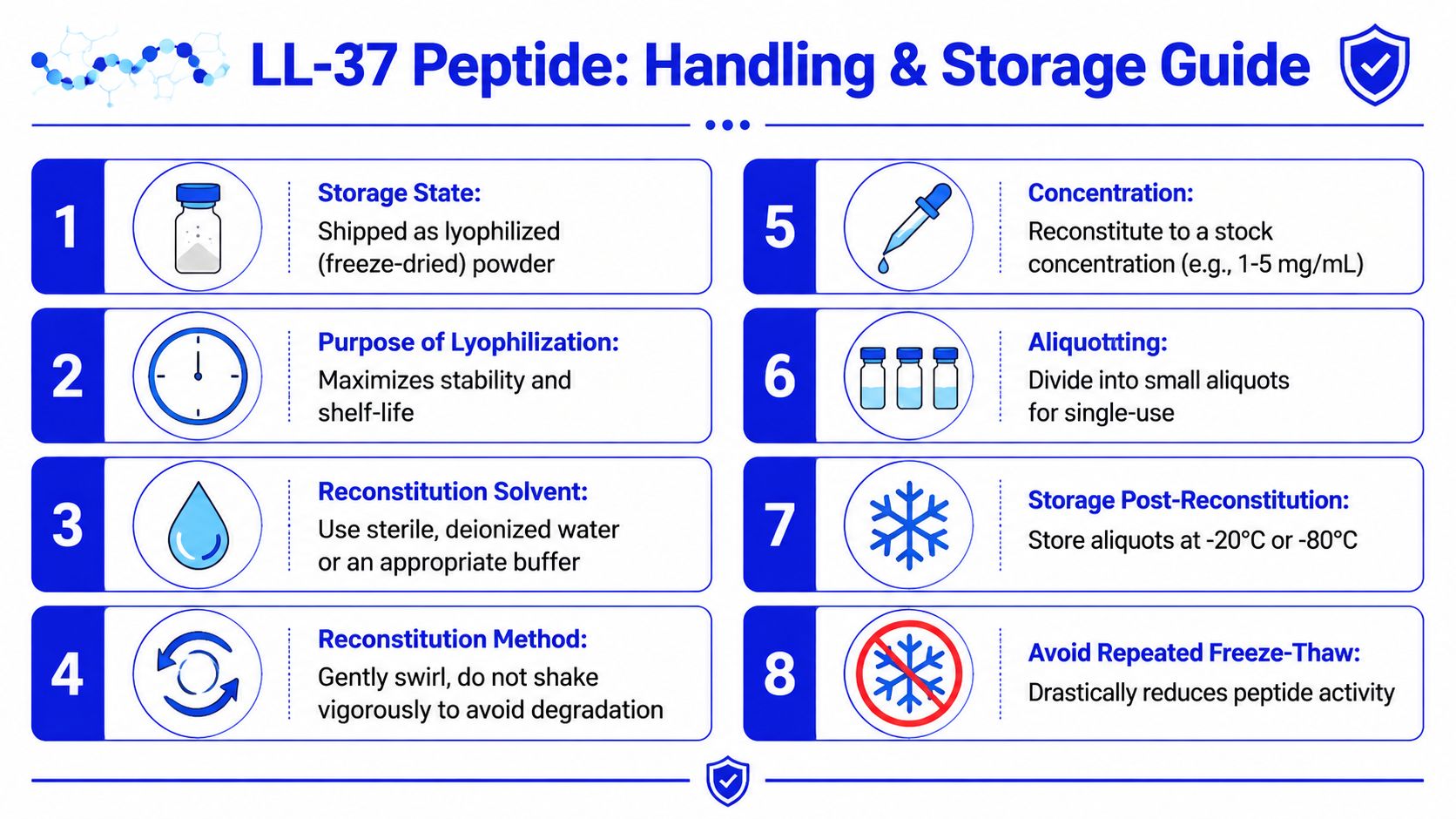
Reconstitution sounds simple, but small handling choices can affect reproducibility. The priority is to create a solution that is accurately concentrated, minimally stressed, and easy to aliquot.
General best practices include:
A useful handling video appears below.
Researchers often ask whether higher concentration stock solutions are always better. Not necessarily. A highly concentrated stock can be convenient, but only if it remains workable for accurate dilution and compatible with the assay matrix.
Use this checklist before running a study:
The human topical data mentioned earlier offers one good conceptual reminder. In the chronic leg-ulcer study, 0.5 mg/mL and 1.6 mg/mL improved outcomes, while 3.2 mg/mL did not show statistically significant benefit, based on the earlier linked PubMed study. Handling and formulation don’t replace biology, but they can either preserve or blur the concentration window you’re trying to study.
A Certificate of Analysis, or COA, is one of the few documents in peptide procurement that directly affects scientific confidence. If a lab can’t verify what arrived in the vial, every downstream result becomes harder to interpret.
A useful LL-37 COA should help a researcher answer three questions.
First, is it the right peptide?
Identity is commonly supported by mass spectrometric confirmation or equivalent analytical identity testing.
Second, how pure is it?
Purity is often reported by HPLC or a similar chromatographic method. Higher purity generally reduces the chance that side peaks or synthesis-related impurities are driving unexpected assay behavior.
Third, does the lot match the paperwork?
Lot number alignment sounds basic, but it’s essential for traceability and reproducibility.
A quick review checklist:
Researchers sometimes treat COAs as purchasing paperwork. That’s too casual. A COA is part of the experimental record.
If one batch behaves differently from another, lot-level documentation may explain why. If a paper or internal report needs to be repeated months later, traceable analytical data gives the team a baseline for comparison. Without that, it’s difficult to tell whether the biology changed or the material changed.
LL-37 sold by research suppliers is intended strictly for laboratory, analytical, and preclinical research use. It is not a drug, supplement, or approved medical product for human or veterinary use.
That boundary isn’t a technicality. It affects how the material should be purchased, stored, documented, and handled. Researchers should use appropriate PPE, maintain clean technique, follow institutional protocols, and keep records that support traceability and safe laboratory practice.
LL-37’s dose-dependent behavior makes disciplined handling even more important. A compound with context-sensitive effects shouldn’t be treated casually.
The search for a universal LL-37 peptide dosage usually ends in frustration because the question is too broad. LL-37 doesn’t behave like a one-number compound. Its meaning changes with concentration, route, local exposure, tissue environment, and model type.
The strongest human evidence remains in topical wound research, where 0.5 mg/mL and 1.6 mg/mL outperformed placebo, while 3.2 mg/mL did not, according to the earlier linked clinical study. Outside that setting, the literature becomes more fragmented, with broader animal dosing ranges and much less standardization. That’s why serious research starts with model-specific reasoning, not copied protocols.
Good LL-37 work depends on four things: choosing the right exposure range, keeping units straight, handling the peptide carefully, and verifying lot quality with proper documentation. If those pieces are in place, your data will mean far more than a guessed “dose” ever could.
For your next study, learn more about Peptide Warehouse USA and explore research-grade peptide options backed by transparent batch documentation, third-party testing, and a research-use-only supply standard built for laboratory reproducibility.



