No products in the cart.

You’ve probably seen the same pattern many researchers see now. A peptide gets discussed in forums, podcasts, supplier catalogs, and conference side conversations long before the average reader has time to trace the actual literature. With BPC 157 & TB 500, that gap between conversation and evidence is exactly where confusion starts.
The compounds are usually described as “recovery” or “repair” peptides, but those labels blur several important distinctions. BPC-157 is discussed mostly through preclinical healing models and a very small amount of human data. TB-500 is usually discussed through the biology of thymosin beta-4, plus animal work and anecdotal use, even though TB-500 itself is not FDA approved. For anyone doing legitimate laboratory or preclinical work, the right question isn’t whether the hype sounds plausible. It’s whether the underlying evidence, mechanism, and material quality justify careful study.
This guide takes a pragmatic view. It treats BPC 157 & TB 500 as research compounds, separates mechanism from marketing, and focuses on what matters in practice: what each peptide is, why people study them together, where the human evidence remains thin, and how sourcing and batch documentation affect research quality.
A common research scenario starts the same way. A lab wants to study soft-tissue repair or recovery biology, and two peptide names keep appearing in papers, forums, and supplier catalogs: BPC 157 and TB 500.
The problem is not lack of interest. It is signal-to-noise. Discussions around these compounds often mix animal findings, mechanistic hypotheses, anecdotal claims, and uneven product quality as if they carry the same weight. They do not.
For research purposes, the useful starting point is simple. Treat BPC 157 and TB 500 as experimental compounds with intriguing preclinical signals, limited human evidence, and a high need for careful interpretation. That distinction matters because a rodent healing model and a controlled human clinical dataset answer different questions. One can suggest biological plausibility. The other is needed before anyone can speak confidently about human outcomes.
A practical way to frame the topic is to separate three layers of evidence. First, what has been observed in preclinical models. Second, what has been studied in humans, which remains sparse. Third, whether the material used in a study is sufficiently characterized to make the results worth trusting. A promising peptide with weak analytical documentation is a bit like a clean assay run with an unverified standard. The readout may look precise, but the foundation is uncertain.
That is why this guide takes a pragmatic research view rather than an optimistic marketing view. The goal is to explain what these compounds are, where the evidence is strongest, where it is thin, and how sourcing discipline, including certificates of analysis and independent testing, shapes the quality of any serious laboratory work.
One working rule helps keep the discussion grounded.
Working rule: If a peptide has broad mechanistic appeal but little clinical depth, the quality of your interpretation matters as much as the quality of the vial.
Used this way, the topic becomes much clearer. Interest in BPC 157 and TB 500 may be reasonable in experimental settings, but broad conclusions require much more than a plausible mechanism or a striking animal result.
A common research scenario goes like this. A peptide is described online as a broad healing agent, the mechanistic language sounds plausible, and the human evidence is assumed to be stronger than it is. BPC-157 deserves a more careful read than that.
BPC-157 is generally presented as a synthetic peptide associated with a gastric protein context, which is why discussions often center on gastrointestinal protection and connective tissue repair. For a laboratory researcher, the more useful question is narrower. What has been observed in controlled preclinical models, and what remains unsettled because human data are sparse?
Most of the literature sits in preclinical work. Researchers encounter BPC-157 mainly in animal and translational models that examine tendon, ligament, muscle, bone, and gastrointestinal injury responses, rather than in large, well-controlled human trials.
That distinction matters. Animal studies can show that a compound changes repair-related biology under defined conditions. They do not, by themselves, establish clinical benefit, optimal dosing, or long-term safety in humans.
Across the preclinical literature, several themes appear repeatedly:
A practical analogy helps here. In an injury model, blood supply functions like delivery routes, fibroblasts function like site crews, collagen functions like structural material, and adhesion signaling helps coordinate where the crews and materials go. That framing is useful for understanding why BPC-157 continues to attract experimental interest even though the clinical literature remains limited.
A visual overview can help if you want a quick refresher before going deeper:
Mechanistic language can create false confidence if it is not tied to evidence level. A signal in angiogenesis, fibroblast behavior, or adhesion pathways means researchers have a testable biological hypothesis. It does not mean the compound has been validated for clinical use.
That is the key interpretive point with BPC-157. The peptide has a substantial laboratory narrative built from recurring animal findings, especially in injury-repair settings. The human evidence base is still thin, so strong real-world claims outrun what the published record can support.
This is also where sourcing discipline becomes part of scientific judgment. If a compound is being studied mainly through preclinical models, the quality of the material matters even more. Poorly characterized peptide lots can blur whether a result reflects BPC-157 itself, impurities, degradation products, or concentration errors. For legitimate laboratory work, certificate of analysis review and independent purity testing are part of the experiment, not an afterthought.
One more point helps prevent category confusion. BPC-157 is often discussed alongside peptides tied to immune or thymic biology, but those are different biological contexts. If you want background on that separate area before comparing compounds, understanding the thymus gland is a useful primer.
The most defensible summary is simple. BPC-157 is a research peptide with repeated preclinical signals in repair-oriented models and limited human validation. It is interesting, but it is not settled.
A common lab scenario goes like this. A protocol mentions TB-500, the supporting paper discusses thymosin beta-4, and the two names start to blur together. That is the first point to correct. TB-500 is generally described as a synthetic analog or fragment associated with thymosin beta-4 biology, not the full native peptide itself.
The confusion starts with shared biological themes. Thymosin beta-4 has been studied in relation to actin binding, cell migration, angiogenesis, and tissue remodeling. Those functions matter because repair is not only about making new tissue. Cells also have to move to the right place, change shape, and reorganize the local environment. Actin is part of that machinery, much like the internal framework that lets a cell shift position and do mechanical work.
That mechanistic link explains the interest in TB-500. Researchers are asking whether a compound tied to thymosin beta-4 biology might influence the kinds of processes that appear in wound-healing and recovery models. The key interpretive point is narrower than many blog posts suggest. A plausible mechanism gives researchers a reason to test a compound. It does not establish clinical benefit in humans.
Human evidence needs especially careful wording here. A science review summary from Spectrum Healthcare describes early clinical work involving thymosin beta-4, while also noting that TB-500 itself is not FDA approved and is still discussed mainly through animal research and anecdotal use claims. That distinction matters because results for thymosin beta-4 cannot be copied over automatically to TB-500.
For readers who want broader biologic context around thymic function and immune relevance, understanding the thymus gland is a useful background primer.
The most useful way to frame TB-500 is as a hypothesis-driven research tool. In preclinical discussions, it is often associated with migration, remodeling, and system-level recovery biology rather than highly localized repair signaling. That framing helps explain why it appears so often in combination discussions, but the evidence base for those broader claims remains limited.
A careful researcher separates three layers of evidence:
That hierarchy helps prevent a common mistake. Mechanistic relevance can make a compound scientifically interesting long before it becomes clinically interpretable. For TB-500, the gap between those stages is still large.
For research purposes, the defensible summary is straightforward. TB-500 is a synthetic peptide analog linked conceptually to thymosin beta-4 pathways, especially those involving cellular movement and remodeling. The preclinical rationale is real. Direct human evidence for TB-500 remains limited, so strong efficacy or safety claims in people go beyond what the published record currently supports.
A researcher setting up an injury model often faces a practical choice. Should the study focus on a peptide associated with more localized repair signaling, or on one discussed in connection with cell movement and broader remodeling biology? That is the value of comparing BPC-157 and TB-500 side by side.
The pair is often discussed together because their proposed roles are different, not because the evidence shows they produce the same effects. In preclinical reasoning, BPC-157 is usually placed closer to tissue-focused questions such as tendon, ligament, muscle, or gut-associated repair models. TB-500 is more often framed around actin dynamics, migration, and system-level remodeling concepts linked to thymosin beta-4 biology.
That distinction matters because a mechanistic fit is only the starting point. It does not establish clinical efficacy, and it does not prove that combining the two creates a synergistic effect in humans.
| Characteristic | BPC-157 | TB-500 (Thymosin Beta-4 Fragment) |
|---|---|---|
| General identity | Synthetic peptide commonly discussed as a body protection compound | Synthetic analog or fragment associated with thymosin beta-4 biology |
| Primary research interest | Tissue-repair signaling in tendon, ligament, muscle, bone, and related models | Cell migration, remodeling, angiogenesis, and recovery-oriented biology |
| Mechanistic themes | Angiogenesis, fibroblast activity, collagen synthesis, FAK-paxillin signaling | Actin regulation, cell migration, stem-cell movement, reduced scar formation |
| Evidence profile | Strongest in preclinical and translational work | Strongest in animal work and extrapolation from thymosin beta-4 biology |
| Human evidence | Very limited | Very limited for TB-500 itself |
| Regulatory status | Not approved for human therapeutic use in this context | Not FDA approved |
One way to read this table is to ask what each compound is helping you test.
If the model is centered on local matrix organization, tendon-to-bone healing, fibroblast behavior, or site-specific repair responses, BPC-157 often fits the experimental question more directly. If the model is built around migration, cytoskeletal dynamics, angiogenic signaling, or tissue remodeling across a wider biological context, TB-500 may be the more natural candidate.
An analogy helps here. BPC-157 is often discussed like a tool for examining what happens at the worksite. TB-500 is more often treated like a tool for examining how cells move through the larger construction zone. Both ideas come from preclinical reasoning. Neither should be mistaken for established human therapeutic performance.
The evidence base also differs in a way that can confuse newer researchers. BPC-157 has a more recognizable literature trail in injury and repair-oriented preclinical models, with limited human discussion at the margins. TB-500 draws much of its scientific interest from the broader thymosin beta-4 literature, then extends that interest to the synthetic fragment used in research settings. That makes extrapolation a central issue. A pathway can be biologically plausible without the specific compound being well validated in people.
For a serious lab, the comparison should narrow claims, not expand them. The careful conclusion is simple. These peptides are discussed as potentially complementary research tools with different mechanistic emphases, but direct human evidence remains sparse, and claims about stacking, recovery, or safety in people go beyond what current published support can firmly establish.
The regulatory status of these compounds isn’t a footnote. It changes how a responsible lab should think about procurement, labeling, study design, and communication.
Neither BPC-157 nor TB-500 should be discussed casually as if they were established therapeutic agents. In the present context, the correct framing is laboratory or preclinical use only.
That’s not just conservative wording. It reflects real concerns about approval status and supply-chain quality.
A medical commentary from Sanctuary Wellness Institute warns that unapproved peptides sold as “research chemicals” can be contaminated or mislabeled, and it further notes that both BPC-157 and TB-500 are on the FDA’s list of substances that cannot be used in compounded drug products. For researchers, that means the phrase “research use only” should be treated as a serious boundary, not a marketing line.
Even if a mechanism looks promising on paper, contaminated or misidentified material can invalidate your work before it starts.
The risk isn’t only about purity percentage. It also includes:
If a vial arrives with weak documentation, your experiment inherits that uncertainty.
Many discussions about the “benefits of peptides” become too abstract at this point. In actual research operations, safety and quality control begin before the first assay, animal protocol, or storage step.
A peptide can sound impressive in theory and still be unusable in practice. For serious research, sourcing is part of the method, not just part of procurement.
The minimum expectation is documentation that lets you evaluate what’s in the vial and how that conclusion was reached.
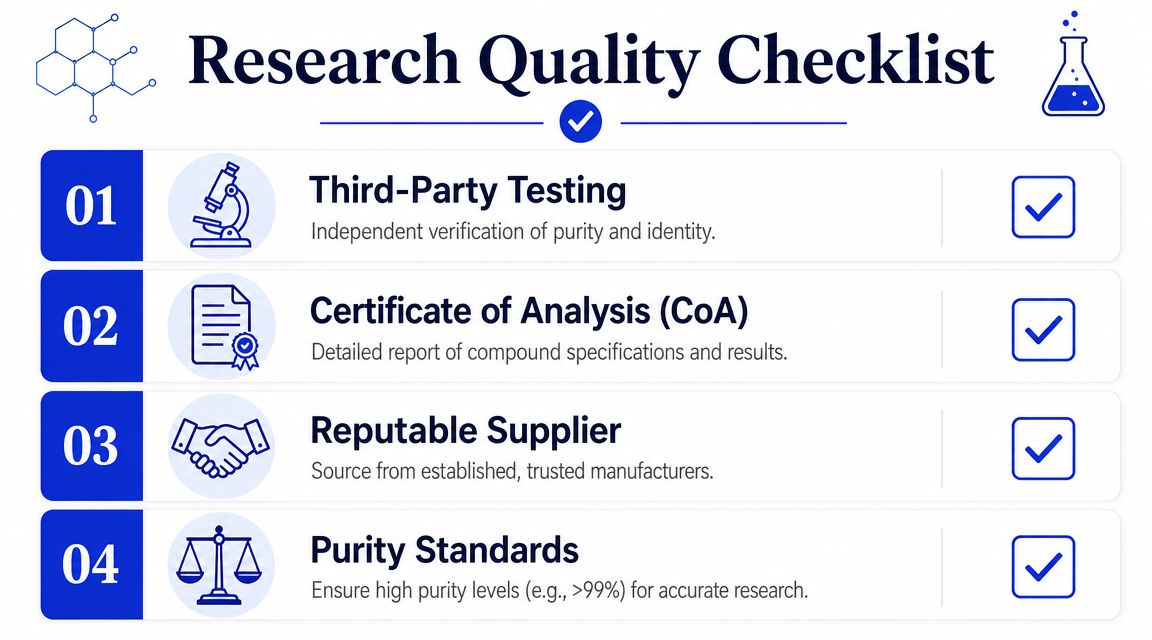
A useful intake checklist includes:
Some suppliers now structure their research catalogs around those expectations. For example, Peptide Warehouse USA states that its research peptide lots are supported by third-party documentation including COAs, microbial and endotoxin reports, and stated purity values for laboratory, analytical, and preclinical use only.
For a broader manufacturing and documentation mindset, this complete guide for fitness professionals is helpful because it explains quality assurance thinking in plain terms that still map well to technical procurement decisions.
Researchers often ask what a COA proves. The answer is narrower than many assume.
A Certificate of Analysis generally tells you what was tested for a specific lot and what result was obtained under the stated method. It doesn’t replace your own handling controls, and it doesn’t prove fitness for every possible use case.
Focus on these details:
Practical screening question: Could another researcher in your lab review this paperwork and reach the same conclusion about identity and suitability?
If the answer is no, the documentation isn’t strong enough.
Good peptide handling starts with boring discipline. That’s usually what protects data quality.
Many research peptides are supplied as lyophilized powder, meaning the material has been freeze-dried to improve storage stability before reconstitution. In practical terms, that gives the lab a dry, more stable starting form, but only if the material is stored and reconstituted carefully.
Basic handling habits matter:
Researchers also get confused about “blends” versus separate vials during method planning. A blend may be convenient for inventory simplicity, but separate vials can offer more control when the goal is to isolate compound-specific effects or preserve flexibility in study design.
Because the human evidence is limited, protocol quality matters even more in preclinical work. If you’re studying BPC 157 & TB 500, define the biological question as tightly as possible.
That usually means being explicit about:
A stronger protocol often comes from subtraction. Cut vague endpoints. Separate mechanism questions from outcome questions. Keep the sourcing record tied to the data record.
Cleaner peptide research usually comes from tighter experimental definitions, not from adding more compounds.
Not necessarily. A blend may simplify handling, but separate vials allow more control over experimental design, sequencing, and compound-specific interpretation. If your study needs cleaner attribution of effects, separate materials are often easier to justify.
It means the peptide has been freeze-dried into a powder for storage before reconstitution. Labs prefer lyophilized material because it’s easier to store and transport than a pre-mixed liquid, but stability still depends on correct handling after reconstitution.
There isn’t a single standard answer. The timeline depends on the tissue model, the biological endpoint, and whether you’re measuring early signaling behavior or later structural change. The safest approach is to let the model and endpoint drive the duration, not online protocol folklore.
Documentation quality, lot traceability, contaminant screening, and clarity about research-only status. Price and convenience matter less if the supporting paperwork can’t defend the material you used.
If you’re evaluating BPC 157 & TB 500 for laboratory, analytical, or preclinical work, start with the evidence, then verify the material. Peptide Warehouse USA offers research-use-only peptides with lot-specific documentation, including COAs and supporting testing details, so you can explore options with a clearer view of sourcing and traceability.



