No products in the cart.
Why do researchers combine two growth hormone secretagogues that act upstream of the same pituitary output instead of choosing the strongest single agent and stopping there?
That question gets missed in most discussions of the Sermorelin Ipamorelin blend. Public-facing descriptions usually stop at “synergy,” but that word doesn’t explain the actual experimental logic. A researcher wants to know which receptor systems are being engaged, what kind of pulse pattern the pairing is intended to produce, how protocols are typically structured, and where the evidence is solid versus speculative.
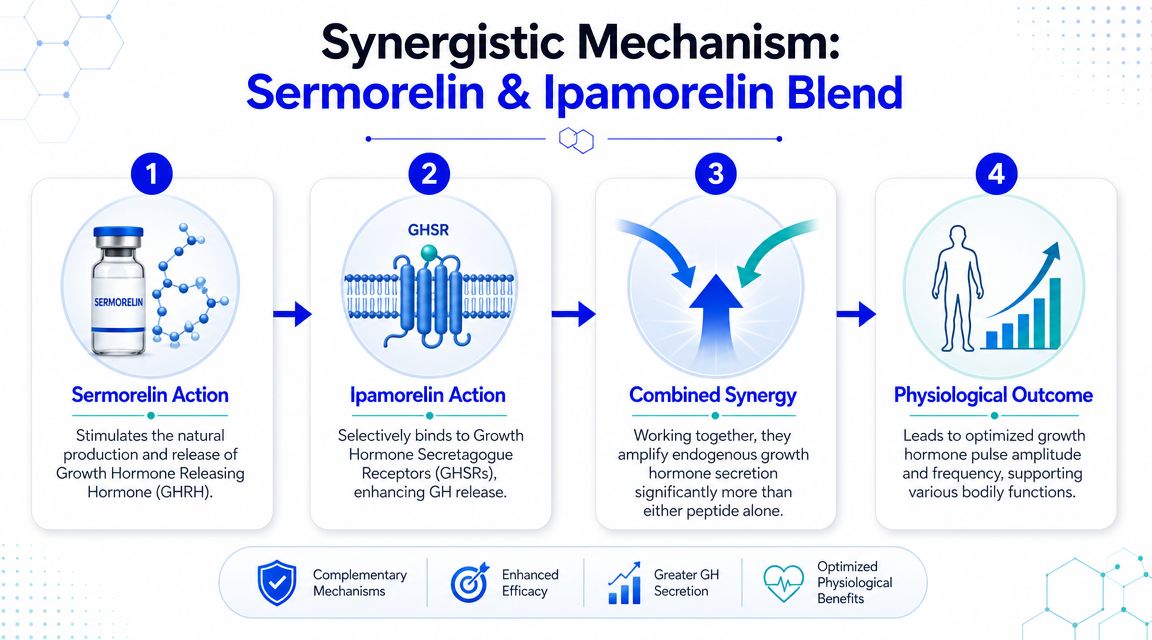
The blend sits in a useful middle ground between simple mechanistic theory and practical peptide protocol design. Sermorelin functions on the GHRH side of the axis. Ipamorelin acts through the ghrelin or GHS-R side. Put together, the pair is used to stimulate endogenous growth hormone release through two different upstream signals rather than supplying exogenous HGH directly.
That distinction matters. For labs interested in sleep, recovery, body composition, age-related GH decline, or endocrine signaling models, the central question isn’t just whether the blend can increase GH-related output. It’s whether dual-pathway stimulation gives a better experimental tool than single-pathway stimulation alone.
Why use a blend at all if each peptide can stimulate growth hormone release on its own?
The answer is mechanistic, not promotional. A single secretagogue gives the pituitary one upstream instruction. A Sermorelin Ipamorelin blend gives two distinct instructions that converge on the same output, GH release, while still relying on the endogenous axis rather than supplying exogenous GH directly.
That distinction matters in research design. If the goal is to raise circulating GH, direct replacement is one model. If the goal is to study how the pituitary responds when two physiologic control inputs are engaged together, a blend becomes a different kind of tool.
Sermorelin provides the GHRH-side signal. Ipamorelin provides the ghrelin receptor-side signal. Those are not interchangeable inputs. They are better understood as two control knobs on the same system, with overlapping downstream effects but different receptor biology, different timing characteristics, and different implications for pulse formation.
This is why researchers often choose the blend over a single agent. The rationale is not redundancy. It is selective coverage of two regulatory pathways that normally participate in GH pulsatility. In practical terms, that can make the blend more informative than sermorelin alone or ipamorelin alone when the question concerns pituitary responsiveness, pulse architecture, or preservation of feedback control.
Sermorelin also has a longer historical and clinical context than many experimental peptides, including prior FDA-approved use in pediatric settings and diagnostic testing, with later discontinuation of the branded product, as noted earlier. That history does not prove superiority of a blend. It does show why sermorelin remains a recognizable reference point in GH-axis research and why it is often used as the anchor peptide in dual-secretagogue protocols.
A common point of confusion is the assumption that combining two GH secretagogues is equivalent to doubling the same signal. It is closer to stimulating the same endocrine output through parallel upstream circuits. If one peptide is best viewed as setting the hypothalamic style of instruction, the other acts more like a separate permissive cue that can amplify release without becoming GH itself.
Practical rule: Researchers usually choose the blend when they want to study endogenous GH secretion under dual-pathway stimulation, rather than model direct HGH replacement.
So the useful question is narrower and more scientific. Under what conditions does dual-receptor stimulation produce a cleaner, more reproducible, or more physiologically relevant GH response than a single-pathway design? That is the underlying rationale for combining sermorelin and ipamorelin.
A useful way to separate these peptides is to ask a narrow mechanistic question: which receptor system is each one meant to stimulate, and what does that let you test?
Sermorelin is a 29-amino acid synthetic analogue of GHRH. A published PubMed review on sermorelin describes its use in diagnostic testing for growth hormone deficiency at an intravenous dose of 1 microg/kg, and also reviews once-daily subcutaneous use at 30 microg/kg in some prepubertal children with idiopathic GH deficiency.
That history matters for experimental design because sermorelin functions upstream of GH. It does not replace GH. It stimulates the GHRH receptor and therefore tests whether the pituitary will respond to a hypothalamic-type release signal.
In a blend, sermorelin is usually the more physiologic organizing input. It asks whether the somatotroph can still respond through the canonical GHRH pathway. For a researcher, that is different from asking only whether GH output can be pushed higher by any available secretagogue.
Ipamorelin is a 5-amino acid ghrelin-mimetic peptide studied for its selectivity at the growth hormone secretagogue receptor, often called GHS-R. Its role in a protocol is therefore different from sermorelin at the receptor level, even though both can converge on GH release.
That distinction is where many summaries become too simplistic. The point of ipamorelin is not merely “more GH.” The point is that it provides a second upstream input through the ghrelin receptor system, which lets a researcher probe whether GH secretion changes when the pituitary is receiving a ghrelin-like permissive signal rather than a GHRH-like instruction alone.
A lab choosing ipamorelin over another secretagogue is usually trying to keep that signal relatively selective. In practical terms, sermorelin tests the GHRH side of pituitary responsiveness, while ipamorelin tests how the same endocrine output behaves when driven through a distinct receptor channel.
If two compounds lead to the same downstream hormone, they can still answer different experimental questions.
Sermorelin is useful when the protocol needs a cleaner read on GHRH-receptor dependent pituitary responsiveness. Ipamorelin is useful when the protocol needs to add ghrelin-receptor mediated secretagogue tone without collapsing the design into direct GH replacement. The blend becomes attractive when a single-agent design would leave uncertainty about whether the observed response depends on one upstream control circuit or reflects broader secretory capacity.
That is the comparative advantage of the pair. A single agent can show that the GH axis responds. A two-component design can show more about how it responds.
| Attribute | Sermorelin | Ipamorelin |
|---|---|---|
| Peptide type | Synthetic analogue of GHRH | Ghrelin-mimetic peptide |
| Amino acid length | 29 amino acids | 5 amino acids |
| Primary pathway | GHRH-side signaling | Ghrelin or GHS-R signaling |
| Main research role | Pituitary GH pulse initiation through GHRH receptor activity | Selective secretagogue input through ghrelin receptor activity |
| Why it matters in a blend | Provides the GHRH signal | Adds a second upstream pathway |
The shortest accurate summary is this:
Why would a researcher use a blend instead of selecting the cleaner simplicity of a single secretagogue?
The answer is mechanistic coverage. Sermorelin and ipamorelin stimulate GH release through different upstream inputs, so the blend is useful when the protocol aims to test how the somatotropic axis behaves under dual physiologic prompting rather than under one isolated cue. As noted earlier, sermorelin addresses the GHRH side of pituitary stimulation, while ipamorelin adds ghrelin-receptor signaling. That difference is the reason the pair is studied together.
A practical comparison helps. Using sermorelin alone is like testing one control line in a circuit. Using the blend is closer to testing whether the system responds differently when two native regulatory lines are active at the same time. For a research design, that can matter more than asking whether GH rises at all.
In strict experimental language, synergy should not be treated as a vague promise of “more.” It refers to the possibility that coordinated activation of the GHRH receptor pathway and the GHS-R pathway produces a response pattern that differs from single-pathway stimulation in timing, amplitude, or reproducibility of pulses.
That distinction matters because GH biology is pulsatile. A protocol built around endogenous secretagogues is often less interested in constant stimulation and more interested in whether pulse generation remains organized. The blend is therefore chosen in studies where pulse architecture is part of the question, especially if the investigator wants to preserve the logic of upstream signaling rather than move to direct GH administration.
Another way to state it is this: the comparative benefit of the blend is not receptor saturation. It is broader interrogation of the regulatory network.
Here’s the video overview referenced in many high-level discussions of peptide combinations:
Timing is part of the mechanism. Researchers often place secretagogue protocols near the normal nocturnal window of GH release because the aim is to interact with an existing physiologic rhythm, not to flatten that rhythm into continuous exposure.
That is one reason bedtime administration appears so often in research-oriented discussions of sermorelin and ipamorelin. The logic is straightforward. If endogenous GH output already tends to concentrate around sleep onset and early sleep stages, a dual-pathway protocol placed in that window may give a clearer read on secretory responsiveness than the same protocol placed at an arbitrary daytime interval.
Three design implications follow:
Used this way, the sermorelin ipamorelin blend is less about making a broad claim of synergy and more about choosing a protocol that matches the biology being studied.
The evidence base is strongest when the claim stays narrow. Reviews show that sermorelin can raise GH and IGF-1, and some literature suggests it may improve lean body mass. That gives researchers a legitimate reason to treat sermorelin as more than a theoretical component in the blend.
There’s also a clear historical and technical basis for viewing the blend as part of a broader move toward endogenous GH secretagogue strategies. That framing is reasonable because sermorelin has regulatory history and ipamorelin contributes a distinct ghrelin-receptor signal.
A fair reading of the literature supports this statement: the blend has a coherent mechanism, and that mechanism aligns with common research interests in sleep, recovery, body composition, and age-related GH decline.
The harder question is the one most readers care about. Is the blend meaningfully better than using either peptide alone?
The answer is that public-facing comparative outcome data are limited. A review of growth-hormone secretagogues notes that while sermorelin can raise GH and IGF-1, longer-term studies are still needed, and body weight and body fat were unchanged in at least one longer-term context. The same review highlights that the incremental benefit of a blend over a single agent remains a key open question, as discussed in the PMC review of growth-hormone secretagogues.
A mechanistic rationale is not the same thing as a comparative outcome dataset.
That distinction matters for protocol design. If a lab chooses the blend, it should do so because the experiment requires dual-pathway stimulation, not because comparative superiority has already been settled in the literature.
A balanced takeaway looks like this:
What question is the protocol built to answer?
That should be settled before dose selection, because the sermorelin ipamorelin blend can be used to study several different phenomena that look similar on paper but require different designs in practice. A mechanism study asks whether dual receptor-level input changes pulse behavior or downstream signaling. A comparative study asks whether the blend produces a different response than sermorelin alone or ipamorelin alone. A timing study asks whether the same blend behaves differently when administration is aligned with expected nocturnal GH activity versus another window.
Published and research-oriented protocols often place the blend in a low-microgram range per component, with bedtime scheduling used when the goal is to model physiologic pulsatility. As noted earlier, clinical sermorelin literature also provides a general frame for daily dosing and IGF-1 follow-up. Those numbers are a starting point, not a template.
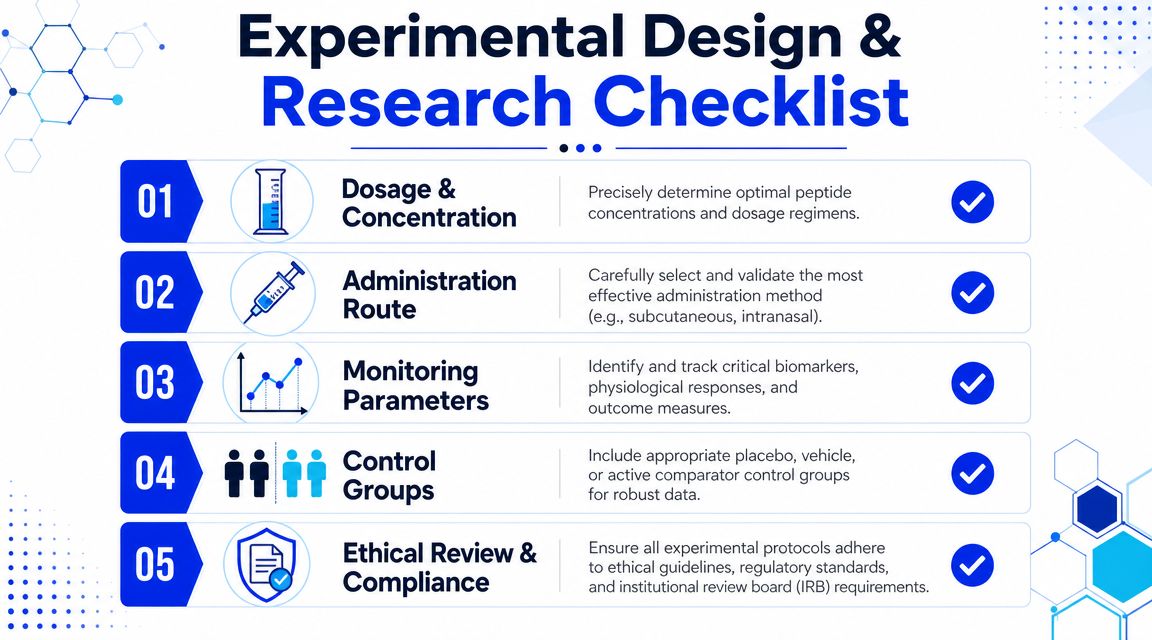
The more important design choice is why the blend is being used at all. If a lab selects two agents, the protocol should test the consequence of combining a GHRH analog with a ghrelin-receptor agonist, rather than treating the blend as a single black box intervention. In plain terms, adding ipamorelin should answer a specific question about amplitude, consistency, timing, or responder profile. If that question is missing, a single-agent arm may have been the cleaner experiment.
A practical setup often includes at least one comparator condition:
That structure matters because a blend can increase interpretive complexity as easily as it increases biological activity.
Endpoint selection should follow the mechanistic rationale with very little drift. If the proposed advantage of the blend is better GH pulse recruitment, then endocrine sampling needs to reflect that claim. If the proposed advantage is stronger downstream axis engagement over time, then longitudinal biomarkers become more informative.
IGF-1 is often the easiest downstream marker to follow because it integrates GH-axis activity over time better than a single random GH measurement. It does not answer every question. A protocol focused on pulsatility may need repeated sampling windows or other timing-aware endocrine measures. A protocol focused on phenotype may need body composition, recovery, sleep, or performance-related endpoints, depending on the model and the research setting.
Researchers sometimes choose broad outcome panels to cover every possibility. That approach can blur interpretation. A narrower panel, selected in advance and tied to the hypothesized benefit of the blend, usually produces cleaner conclusions.
A blend is only more informative than a single agent when the endpoint can detect what the second signal was expected to change.
Cohort definition does much of the analytical work before the first sample is collected. In GH-axis research, baseline heterogeneity can obscure whether the blend failed biologically or whether the study enrolled subjects with very different endocrine starting points.
For teams refining screening logic, OMOPHub’s inclusion criteria insights provide a useful framework for aligning eligibility rules with the actual endpoint. That is particularly relevant here because age, sleep quality, training load, adiposity, prior peptide exposure, and baseline endocrine status can all affect how a subject responds to secretagogue-based protocols.
Useful criteria usually include:
Good study design reduces ambiguity. For a sermorelin ipamorelin blend, that usually means one thing above all else. Build the protocol so it can show why two signals were used instead of one.

What can distort a blend study before dosing even begins. The answer is often the vial itself, or more precisely, how the researcher interprets what is in it.
Blend products are commonly supplied as lyophilized powder in a fixed sermorelin-to-ipamorelin ratio, often with equal mass assigned to each component, as noted earlier. That fixed ratio matters because reconstitution is not just a storage step. It defines the dose mathematics for the entire protocol. If a researcher records only total peptide concentration after adding diluent, the log may look correct while the per-peptide exposure is still being tracked incorrectly.
A blend behaves like a two-channel reagent packaged in one container. One volume calculation now governs both the GHRH-side input and the ghrelin-receptor-side input. That is convenient operationally, but it also means one arithmetic error propagates across both signals.
Lyophilized peptides usually tolerate routine lab handling well if the process is controlled. Problems arise from repeated small errors, not from a single dramatic mistake. Warm bench exposure during setup, vigorous shaking, inconsistent aliquot volumes, and incomplete labeling can all shift the administered dose away from the intended one.
For blend work, handling discipline has a second purpose beyond preservation. It protects interpretability. If a single-agent study is misreconstituted, one exposure curve is uncertain. If a fixed-ratio blend is misreconstituted, uncertainty enters both components at the same time, and later comparisons against sermorelin-only or ipamorelin-only arms become less convincing.
Useful controls are straightforward:
Those steps sound procedural because they are. They also determine whether the blend remains a defined experimental input or becomes a loosely described mixture.
Quality control starts with identity and traceability, not with appearance. A white lyophilized cake can still be the wrong material, degraded material, or material with incomplete documentation. Researchers should read the Certificate of Analysis and associated batch records as part of the method, not as purchasing paperwork.
The key question is simple. Does the documentation support the claim that the vial contains the stated peptides, at the stated purity, tied to the stated lot, with testing records that fit the study’s risk profile? For some projects, identity and purity are the main concern. For others, microbial burden, endotoxin status, residual solvent data, or stability information may also matter.
Check for agreement across the full record set:
Batch quality is part of the experimental method.
That point matters even more with a sermorelin ipamorelin blend than with a single peptide. The rationale for using the blend is mechanistic precision. If material identity, ratio integrity, or reconstitution records are uncertain, the study no longer tests a dual-pathway design cleanly. It tests a poorly defined intervention, and that weakens every downstream conclusion.
The Sermorelin Ipamorelin blend is most useful when you treat it as a dual-pathway endocrine research tool rather than a catch-all “anti-aging stack.” Sermorelin contributes the GHRH-side signal. Ipamorelin contributes the ghrelin-receptor signal. The value of the pairing comes from combining those inputs to study endogenous GH pulsatility with more nuance than a single-agent design can offer.
That doesn’t mean every blend protocol is automatically better. The current evidence base supports the mechanism more clearly than it proves long-term comparative superiority over either peptide alone. For a researcher, that’s not a weakness. It’s the actual opportunity. The unanswered questions are now easier to define: which populations respond best, which endpoints show the clearest incremental value, and when does a blend justify its added complexity?
The practical side matters just as much as the theory. Good study design, clear comparator arms, disciplined endpoint selection, and rigorous peptide handling all shape whether a blend experiment produces interpretable data. Without that structure, even a sound mechanistic rationale can turn into noisy results.
Future work should focus on direct blend-versus-single-agent comparisons, better patient or cohort selection logic, and tighter alignment between pulse-based mechanisms and measurable outcomes. Researchers who want reliable findings should also prioritize high-purity material, transparent batch documentation, and careful protocol standardization.
If you’re sourcing peptides for laboratory, analytical, or preclinical work, Peptide Warehouse USA offers U.S.-made research compounds with batch documentation, COAs, and transparent testing records to support reproducible peptide studies. Learn more and explore options that fit your research workflow.



