No products in the cart.
Most advice about Noopept nasal spray gets the central issue wrong. It treats the spray as a convenience format, as if moving a compound from a capsule to a bottle were mainly about speed or preference. In a serious preclinical setting, that view creates bad data fast.
A Noopept nasal spray is a delivery system, not a shortcut. If the formulation is weak, the spray pattern is inconsistent, or the solution lacks the right excipients, the route stops being an advantage and starts becoming a source of variability. That matters more with a low-dose neuroactive compound than most online discussions admit.
Noopept itself has a narrow base of published human evidence. The Alzheimer's Drug Discovery Foundation notes that it was developed at the Zakusov Institute of Pharmacology of the Russian Academy of Medical Sciences and has only one published clinical trial in peer-reviewed literature. That alone should push any research team toward stricter controls, not looser ones.
The practical question isn't whether intranasal Noopept sounds efficient. The practical question is whether your formulation, handling, and documentation are good enough to make the route scientifically useful.
Researchers use intranasal delivery for a reason. It can provide rapid access through the nasal mucosa, avoid the gastrointestinal environment, and reduce the practical losses associated with first-pass metabolism. But those benefits only exist when the dosage form is built to support them.
That's the part low-quality content skips. It talks about pumps, bottle sizes, or anecdotal timing, while ignoring release behavior, mucosal retention, excipient compatibility, and batch-level consistency. In real lab work, those variables shape the result more than the bottle format does.
A sound Noopept nasal spray workflow starts with three assumptions:
Practical rule: Treat every intranasal preparation like an analytical instrument. If you wouldn't accept drift, contamination, or poor calibration in a core lab instrument, don't accept it in your spray formulation.
In preclinical work, that mindset changes how teams plan studies. It affects what they buy, how they store it, how they administer it, and how they interpret outliers. A surprising amount of "compound performance" is really formulation performance.
Noopept is often handled online as a category label. In preclinical work, that is a poor starting point. The compound has to be defined as a specific chemical entity, with specific analytical and formulation constraints, before intranasal delivery can be evaluated in a serious way.
Noopept is also known as omberacetam and was formerly called GVS-111. Its research history is tied to Russian pharmacology programs, and that background still shapes how the compound is described in the literature and in supplier documents.
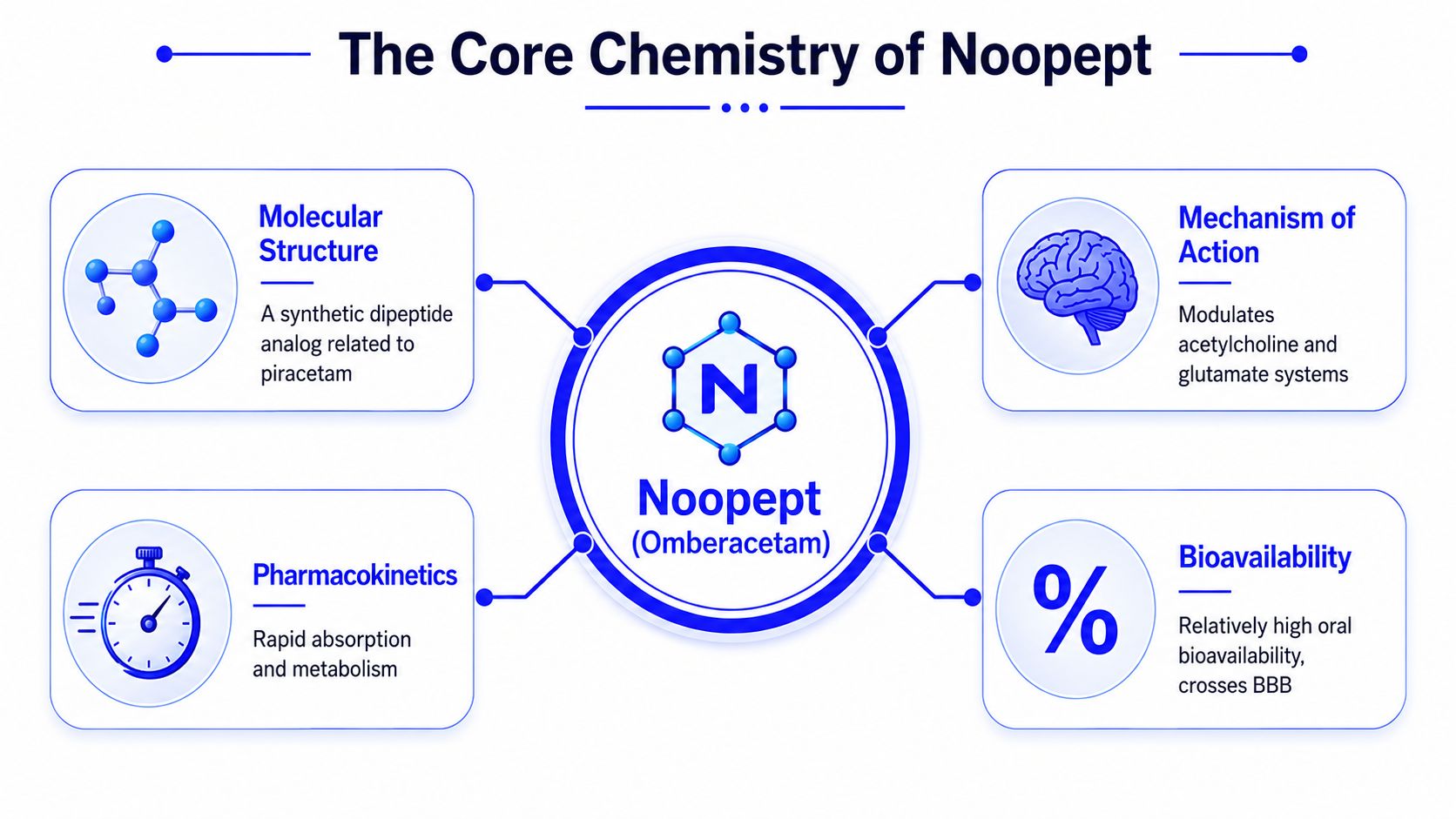
From a laboratory perspective, the relevant question is not whether Noopept is "interesting." The question is whether the material in hand is chemically identified, sufficiently pure, and formulated in a way that preserves reproducible exposure at the nasal surface.
That distinction matters because Noopept is usually discussed through proposed neuroactive effects and its association with BDNF and NGF related pathways. Those terms only become useful in a study design if the compound reaches the intended site with acceptable consistency. If delivered exposure drifts between animals, receptor-level or signaling-level interpretation becomes weak, even when the biological hypothesis is reasonable.
In other words, route selection starts with compound behavior. It does not start with the spray bottle.
Public claims about Noopept are much broader than the published clinical record. As noted earlier, the human literature is narrow, with only limited peer-reviewed clinical evidence available.
One cited open-label study in patients with mild cognitive disorders used 56 days of treatment at 10 mg twice daily and reported improvement in Mini-Mental State Examination scores in the Noopept group. The same summary also described sleep disturbance, irritability, and increased blood pressure in some participants.
For a research team, the lesson is straightforward.
Limited clinical literature should make a lab more careful, not more casual.
The chemistry point is simple. Noopept may justify investigation, but it does not justify loose formulation practice. In intranasal work, weak solvent selection, incomplete dissolution, pH drift, or batch inconsistency can create more noise than the molecule itself.
Intranasal delivery earns attention in preclinical work because it can change the exposure profile in ways oral dosing often can't. The route can move a compound past the GI tract, reduce first-pass metabolic loss, and create a faster path toward central effects when the formulation is appropriate.
That isn't marketing language. It's a pharmacokinetic reason to choose the route.
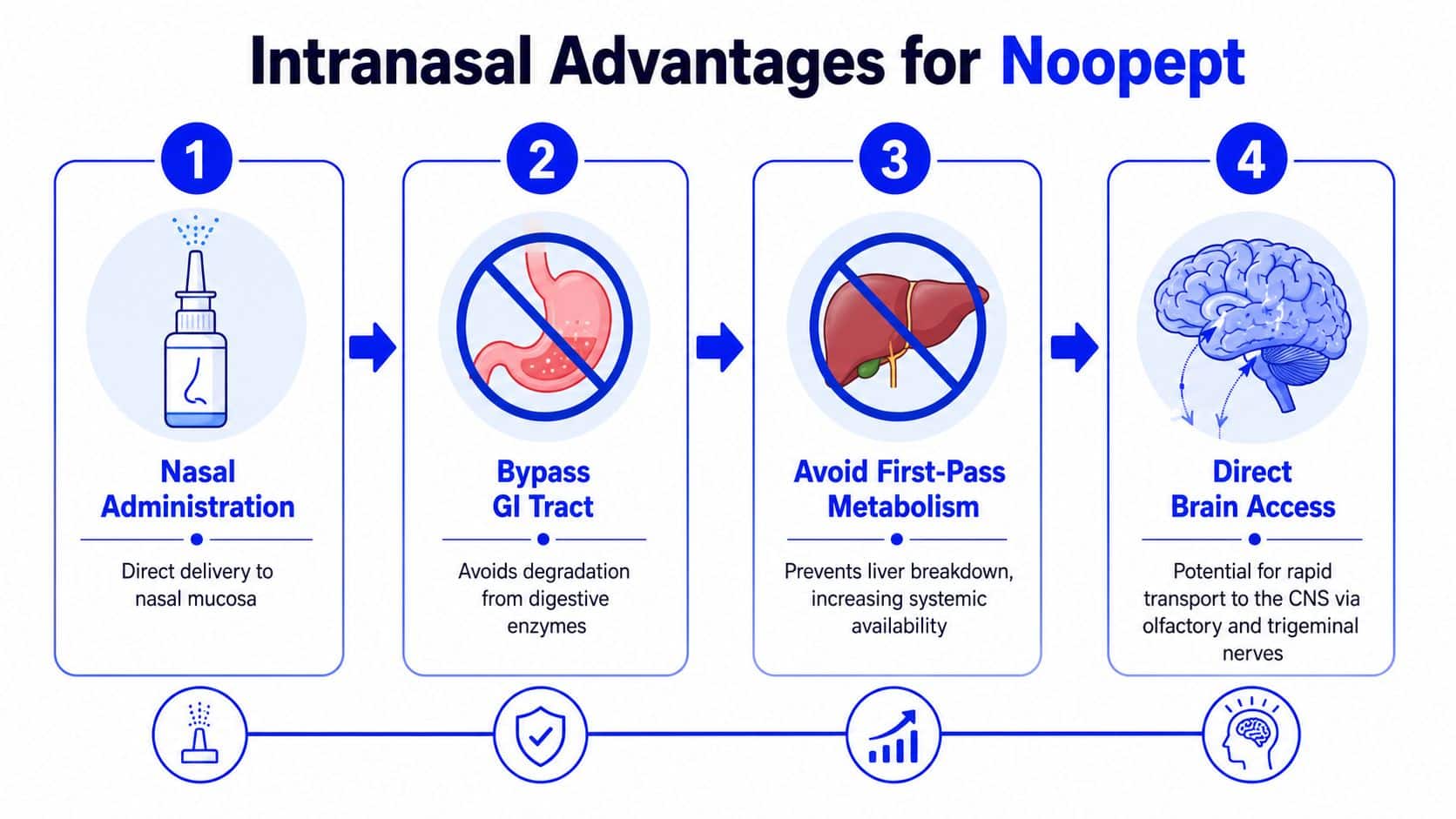
For a research team, the biggest operational advantage is control over variability introduced before the compound even reaches circulation. Oral dosing has to contend with digestive conditions, transit effects, and hepatic processing. Intranasal administration may reduce some of those confounders.
The practical result is often cleaner interpretation of timing-sensitive endpoints. If a protocol depends on behavioral observation windows, neurochemical sampling, or short-interval challenge testing, route-dependent timing matters.
A rat and rabbit pharmacokinetic study of an intranasal Noopept formulation combined with forskolin concluded that it could “bypass the BBB efficiently and achieve high bioavailability in the brain”. In the same line of work, the formulation significantly increased brain BDNF and NGF and was associated with motor and neurodegenerative improvements in PINK1-knockout rats.
That finding supports a specific point. Intranasal Noopept isn't just a bottle-based alternative to oral administration. In the right system, it becomes a route chosen for CNS exposure.
The route has strengths, but it also gets oversold. Researchers sometimes assume that because nasal delivery can be fast, any spray will be effective. That assumption fails when the liquid clears too quickly, releases the active unpredictably, or doesn't maintain adequate mucosal contact.
A good way to think about it is this:
| Route question | Useful research answer |
|---|---|
| Is nasal administration faster in principle? | Often, yes. |
| Does that guarantee better brain exposure? | No. Formulation decides that. |
| Is a simple spray enough for preclinical work? | Sometimes, but not reliably. |
| Can route choice improve data quality? | Yes, if administration and formulation are controlled. |
Researchers also overlook administration technique. A nasal route can reduce one source of variability while introducing another. Device performance, delivered volume, animal positioning, and mucosal condition all affect exposure.
The route is an advantage only when the formulation and administration method deserve it.
For preclinical design, intranasal Noopept makes the most sense when the study needs tighter control over onset, brain exposure, or route-specific mechanistic questions. If the lab can't maintain those controls, oral or other standardized approaches may produce more trustworthy data.
The internet treats intranasal Noopept like a shortcut. In the lab, it is a formulation problem first. If the vehicle is poorly designed, the study is no longer testing Noopept under controlled intranasal conditions. It is testing a variable mixture with uncertain deposition, retention, and release.
A stable nasal spray has to behave like a measured dosage form, not a convenient liquid in a bottle.

The most useful non-commercial formulation work on intranasal Noopept points to excipient selection as a primary control variable. One pharmaceutical study reported that polymers such as sodium carboxymethylcellulose and chitosan with glycerol produced favorable and predictable Noopept release from nasal dosage forms.
That result matters because intranasal performance depends on the matrix, not just the active compound. In practice, researchers need the preparation to remain uniform during the study window, wet the nasal surface consistently, and release Noopept at a rate that does not shift from batch to batch.
A workable vehicle usually has to balance four formulation targets at the same time:
Chitosan and sodium carboxymethylcellulose are relevant because they can modify adhesion and release behavior. Glycerol also affects rheology and handling, which can improve or impair repeatability depending on the rest of the formula.
Research groups often start with a simple aqueous mixture because it is easy to prepare. That approach can be useful for a rough pilot, but it is weak for studies that depend on exposure control.
The usual problems are predictable.
Surfactant level can also shift release behavior. Another formulation study reported that Tween-80 significantly affected Noopept release from nasal dosage forms, with 1% producing the most favorable release profile and higher concentrations offering no meaningful additional improvement. That does not mean 1% is universally correct. It means concentration-response testing for excipients is part of method development, not an afterthought.
This is the trade-off researchers need to face. A thinner liquid may spray easily but clear too fast. A more viscous system may improve residence time but introduce pump variability, incomplete actuation, or poor dose recovery. Better retention is only useful if the formulation still delivers a controlled and reproducible amount.
For preclinical work, the best intranasal Noopept spray is the one with characterized release, stable physical properties, and consistent delivered dose across the full study period.
That standard is higher than what anecdotal online guides suggest. It should be. In a serious preclinical setting, the nasal spray functions as part of the measurement system. If the formulation drifts, the dataset drifts with it.
Even a strong formulation can fail under weak lab practice. Most losses in data quality don't come from dramatic contamination events. They come from routine drift, repeated handling, poor labeling, inconsistent storage, and undocumented deviations.

A preclinical team should handle Noopept nasal spray as a controlled research preparation. That starts with ordinary discipline.
One common mistake is sharing the same bottle across too many operators without a handling log. A spray may still look normal while the delivered amount, cleanliness, or administration technique has drifted.
Storage should prioritize compound integrity and traceability. In practice, that means protecting the preparation from unnecessary heat exposure, excessive light, and uncontrolled bench time. Labs also need clear separation between active-use material and reserve stock.
A simple internal checklist helps:
| Checkpoint | What to verify |
|---|---|
| Container status | Cap secure, no visible leak, no residue buildup |
| Appearance | No unexpected change in clarity or physical character |
| Documentation | Lot and use log current |
| Storage return | Material goes back promptly after use |
Good handling doesn't rescue a bad formulation, but bad handling can ruin a good one.
If a lab sees inconsistent outcomes, handling review should happen early. Researchers often look first at animal variability or model sensitivity. In many cases, the more immediate issue is inconsistent storage return, casual relabeling, or undocumented bottle turnover.
A Certificate of Analysis is part of the experimental record. For intranasal Noopept work, it should be read with the same care given to a dosing log or an analytical method, because any ambiguity at receipt can compromise lot traceability later.
The first question is identity. The COA should state how the material was identified and tie that result to the exact lot in hand. The second is purity. A percentage alone is not enough unless it is batch-specific, dated, and linked to a defined test method. The third is suitability for the intended preparation. For an intranasal research workflow, the review should include any impurity, contamination, or ancillary testing that matters for that formulation and route.
Read the document against the bottle label, purchase record, and internal receiving log. All three should agree. Small mismatches in lot code format, test date, or product description are often dismissed during intake, then become serious problems when a study needs to be reconstructed months later.
A useful COA review asks a short set of technical questions:
The COA also has to be interpreted in context. High purity for the incoming active does not prove that the final nasal preparation will remain uniform, stable, or fit for use under study conditions. It only establishes the starting point.
Preclinical intranasal studies rise or fall on definition and control of the material used. As noted earlier, published formulation work is useful because it shows how tightly specified preparations support interpretable outcomes. The practical lesson for COA review is straightforward. If the batch record is weak, later claims about reproducibility are weaker too.
Many labs frequently lose data integrity without noticing. A team may have a legitimate COA, but then transpose a lot number into a spreadsheet, abbreviate a supplier name inconsistently, or attach the wrong PDF to the receiving record. Those are preventable failures. Groups that digitize incoming quality paperwork and use OCR workflows to reduce manual data entry errors usually maintain cleaner chain-of-custody records and spend less time resolving documentation conflicts during audit or manuscript preparation.
Software helps with extraction and indexing. It does not replace scientific review.
A qualified reviewer should confirm that the COA matches the material type, the intended intranasal formulation, and the protocol-specific use of that lot. If the study depends on comparing lots across time, the review should also document whether test methods or reporting conventions changed between batches.
Reliable preclinical data starts at receiving. The lot must be verified, logged, and matched to the protocol before dosing begins.
Sourcing Noopept for laboratory work requires more than finding an available listing. Researchers need material that is properly designated for research use, backed by transparent documentation, and procured through a supply chain that won't create avoidable compliance problems.
A credible supplier usually makes quality visible before purchase. That means clear batch traceability, accessible analytical documentation, and labeling that supports research inventory control rather than consumer-style marketing.
Useful procurement criteria include:
A practical procurement review should also examine whether the supplier presents the intranasal format as a researched dosage form or merely as a convenience item. That distinction tells you a lot about how seriously the product category is handled.
Noopept isn't an FDA-approved drug in the United States for general clinical use in the context discussed here. For research teams, that means intended use language matters. Materials should be purchased, stored, and documented within a research framework, not treated like consumer wellness products.
When a supplier blurs that line, it creates two problems at once. It weakens scientific confidence in the product, and it makes internal compliance harder for the lab. Clear "research use only" positioning, aligned records, and consistent documentation protect both the study and the institution running it.
A Noopept nasal spray only becomes scientifically useful when the lab treats it as a full delivery system. The compound matters, but the formulation, handling, documentation, and sourcing standards determine whether the resulting data is credible.
That's the main divide between anecdotal online content and serious preclinical practice. Casual advice focuses on convenience. Good research focuses on release behavior, mucosal retention, batch traceability, and reproducibility.
Intranasal delivery can offer real advantages in a model. But those advantages don't come automatically from putting Noopept into a spray bottle. They have to be earned through formulation design and disciplined lab execution.
Researchers who want cleaner outcomes should prioritize documented quality over improvisation, and verified materials over attractive shortcuts. That's especially true with compounds that have a limited published human evidence base and route-sensitive performance characteristics.
If you're sourcing high-purity compounds for laboratory and preclinical applications, Peptide Warehouse USA is worth a closer look. Their catalog includes research-focused nasal sprays and related compounds backed by batch documentation, COAs, and transparent quality practices designed to support traceability and consistency. Explore options and learn more about their research-use supply standards before your next procurement cycle.



