No products in the cart.
Thymosin Alpha-1 research protocols range from 5 to 7 days in some settings to 6 to 12 months in others, and a commonly cited regimen is 1.6 mg by subcutaneous injection twice weekly. That spread exists because the right duration depends on the research objective, not because one protocol is universally “best.”
Those inquiring about Thymosin Alpha 1 how long to take often seek a single cycle length. That's usually the wrong frame. In research, duration follows mechanism, endpoint, and model design.
A short course makes sense when the protocol is testing near-term immune support in an acute setting. A longer cycle makes sense when investigators are studying immune modulation that needs time to stabilize, especially in chronic or recurrent models. If you only copy the headline dose and ignore the reason behind the timeline, the protocol loses its logic.
Thymosin Alpha-1 (TA-1) is generally discussed in research as an immune modulator, not as a simple on-off stimulant. That distinction matters. A stimulant is expected to produce a fast, obvious signal. A modulator is expected to shape how the system responds over time.
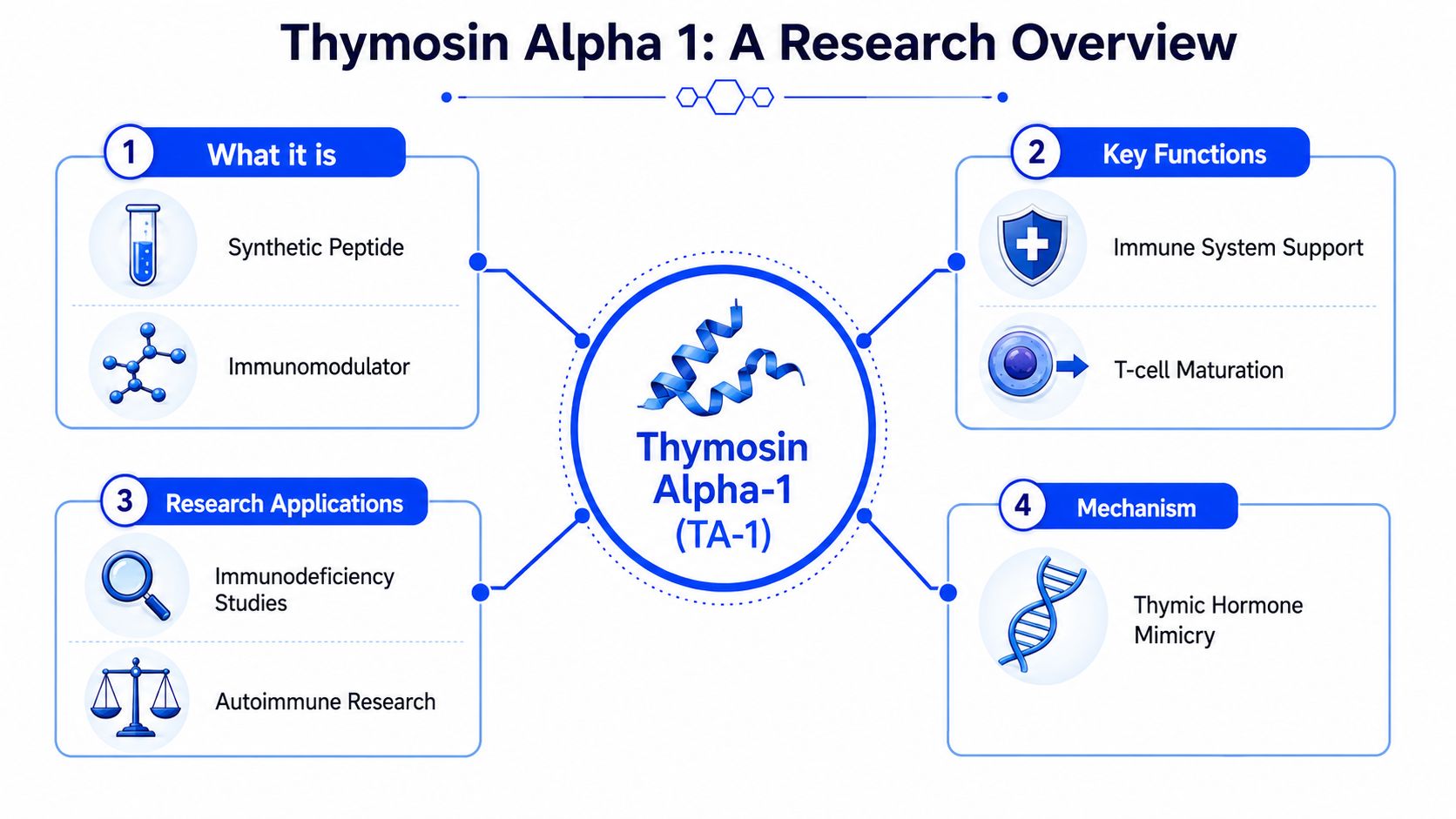
The easiest way to think about TA-1 is as a conductor for an orchestra. It doesn't “play” every instrument itself. It helps coordinate timing, balance, and responsiveness across the immune system.
That's why protocol design often focuses on the quality of the immune response rather than just speed. In research settings, investigators are typically asking whether the system becomes better regulated, better coordinated, or more resilient over a defined period.
A practical implication follows from that mechanism:
Practical rule: If the peptide is being used as a modulatory tool in research, the duration should match the time required for the biological system to show a meaningful shift, not the researcher's preference for a shorter timeline.
TA-1 isn't a new compound in the literature. A monograph notes it has been studied since 1979, with safety reported in more than 3,000 individuals and across over 70 clinical studies. The same monograph also summarizes repeat-dose toxicology findings showing no drug-related adverse effects after 13 weeks in mice, rats, and marmosets at doses up to 6 mg/kg per day, and after 26 weeks at up to 1 mg/kg per day in animal work, which is one reason it remains a serious subject of ongoing inquiry in immune-focused research (A4M thymosin alpha-1 professional monograph).
That history doesn't tell you how long any one protocol should run. It does tell you that researchers have had enough time and enough exposure to move beyond simplistic one-size-fits-all schedules.
Another useful point is conceptual. When a compound has been explored across acute, chronic, and adjunctive contexts, you should expect protocol heterogeneity. Wide variation is not a flaw in the literature. It often reflects that investigators were asking different questions.
The biggest mistake in Thymosin Alpha 1 how long to take searches is treating duration as if it were a property of the peptide alone. It isn't. Duration is a property of the study design.

An acute model asks a short-window question. The protocol may be designed to observe what happens during a narrow period of immune stress or viral challenge. In that setting, a shorter course can be scientifically coherent because the endpoint is near-term.
A chronic model asks a different question. The researcher may want to know whether repeated exposure shifts immune behavior in a more durable way. That kind of question usually needs more time because stable modulation is slower to observe than immediate reactivity.
Many readers often find themselves confused. They see one study using a brief course and another using a much longer cycle, then assume one must be excessive. In reality, the durations may both be appropriate because the endpoints are different.
Frequency tells you how often the peptide is administered. Duration tells you how long the protocol continues. Those are related, but they aren't interchangeable.
Published clinical summaries note that measurable immune-marker improvement is often seen after 4 to 8 weeks of consistent therapy, while more durable benefit may not appear until 3 to 6 months in longer protocols. Those same summaries also frame 4 to 12 weeks as a common reassessment window, which is useful because it shows why investigators often build in review points instead of locking into indefinite continuation (BHR Center clinical summary on thymosin alpha-1).
Early signal and durable effect are not the same endpoint. Good protocol design treats them separately.
That distinction changes how a researcher interprets results. A study might detect movement in biomarkers during the first cycle, yet still need a longer observation period to determine whether the effect persists or translates into the broader endpoint being studied.
A useful way to think about duration decisions:
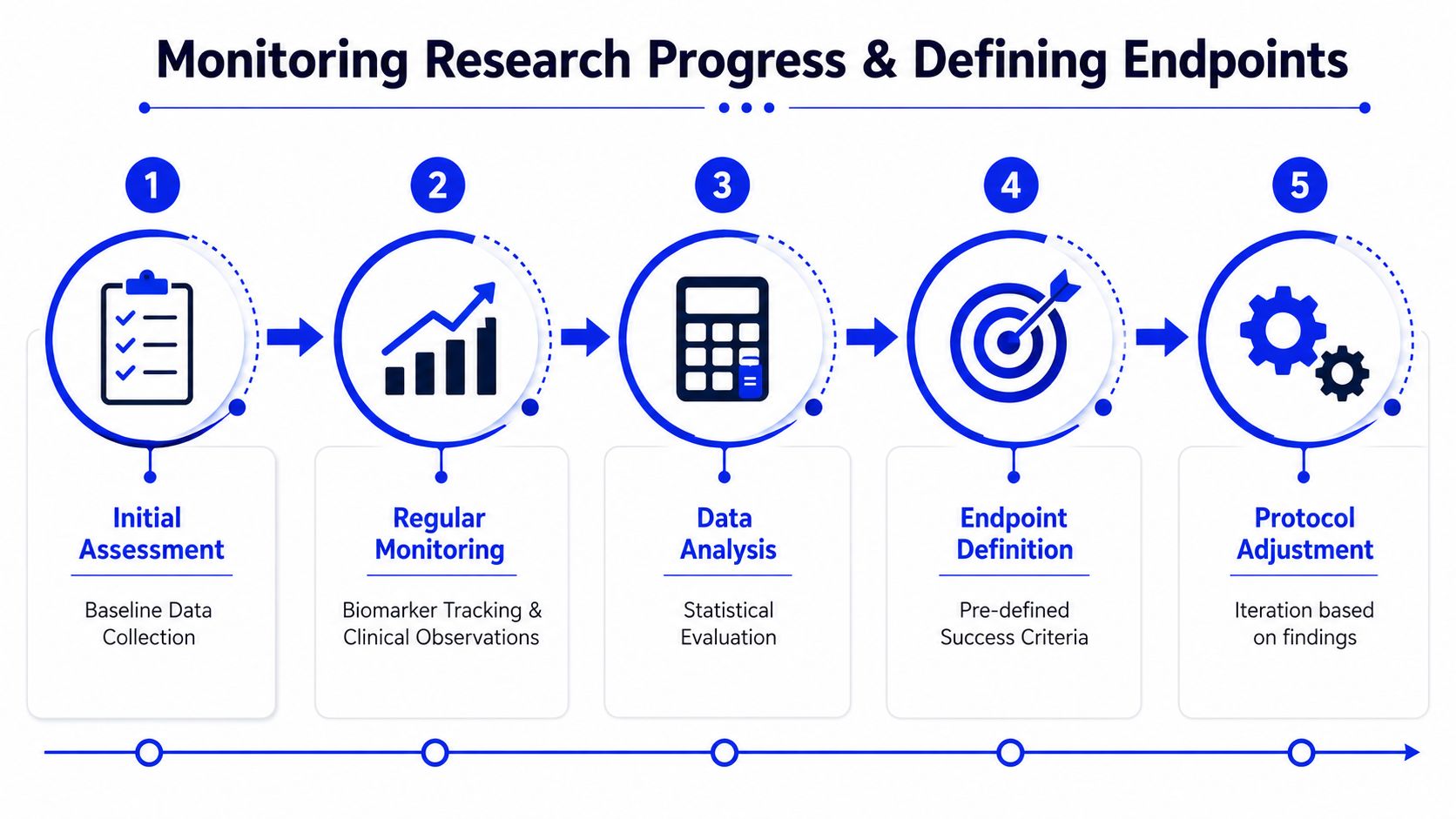
A protocol without predefined reassessment points usually creates confusion. Researchers need a way to decide whether they're observing noise, early movement, or a meaningful pattern.
Here's a concise visual on how investigators often frame those checkpoints in a structured workflow:
The practical trade-off is simple. If you stop too early, you may miss later modulatory effects. If you continue too long without a checkpoint, you risk collecting activity without a clear interpretive framework.
Literature on TA-1 doesn't give one master schedule. It gives a range of protocol patterns tied to context. That range is exactly what researchers should expect from a compound used across different immune-focused study designs.
Published reviews report that a common regimen is 1.6 mg subcutaneously twice weekly, while other protocols include multi-dose courses lasting 5 to 7 days, 5 injections per week for 4 weeks, and in some chronic contexts 6 to 12 months. The same review also notes standard single doses ranging from 0.8 to 6.4 mg, with multiple-dose regimens ranging from 1.6 to 16 mg (published review in PMC on thymosin alpha-1 protocols).
A 5 to 7 day protocol makes the most sense when the question is confined to an acute phase. The study may be asking whether timed administration during a limited biological window changes the near-term response pattern.
That doesn't mean the peptide “works only fast.” It means the study only needed to observe the acute phase.
A protocol using 5 injections per week for 4 weeks sits in a middle ground. It's long enough to move beyond a purely immediate effect, but still structured as a finite cycle with a clear stopping point.
This kind of design is useful when the researcher expects measurable change without committing to a prolonged maintenance-style schedule. It gives enough exposure to watch the direction of biomarker movement, then reassess.
A four-week cycle often functions as a decision point, not a declaration that the peptide's full effect has been captured.
In chronic immune-related contexts, reviews describe regimens lasting 3 months or longer, and in some studies 6 to 12 months. That longer timeline reflects a different hypothesis. The aim isn't just to trigger an early shift. It's to evaluate sustained modulation over a longer biological interval.
For chronic models, that's often the scientifically honest choice. Systems that have been dysregulated for a long period rarely reveal stable directional change in only a few days.
| Research Context | Example Dosage | Example Frequency | Example Duration |
|---|---|---|---|
| Common literature regimen | 1.6 mg | Subcutaneous injection twice weekly | Varies by protocol |
| Acute-phase style protocol | Not uniform across studies | Multi-dose course | 5 to 7 days |
| Intermediate finite-cycle protocol | Not uniform across studies | 5 injections per week | 4 weeks |
| Chronic condition research | Not uniform across studies | Varies by study | 3 months or longer |
| Extended chronic protocol | Not uniform across studies | Varies by study | 6 to 12 months |
A few practical conclusions stand out:
The literature becomes much easier to read once you stop asking, “What's the correct duration?” and start asking, “What biological question forced that duration?”
Duration only matters if the study defines what counts as progress. Without that, a protocol becomes a calendar exercise instead of a research program.
Researchers need endpoint discipline. Before administration begins, the team should decide what outcome would justify continuing, adjusting, or closing the protocol.
For immune-focused TA-1 work, endpoints are usually tied to changes in immune behavior rather than vague impressions. Researchers often monitor trends in T-cell populations such as CD4+ and CD8+, natural killer cell activity, and cytokine patterns. Those markers matter because TA-1 is generally studied as a regulator of immune coordination, so the readout should reflect coordination, not just surface-level observation.
A clear endpoint structure often includes:
Researchers usually combine laboratory markers with operational observations. Biomarkers show biological movement. Observational data help place that movement in context.
That combination matters because immune modulation rarely behaves like a simple binary switch. A marker can improve early, flatten later, or shift in one compartment before another.
Good endpoint design asks two questions at once. Did something change, and did it change in the way the protocol predicted?
Another practical point is consistency. If sampling intervals drift, handling methods vary, or the endpoint gets revised after data begin coming in, interpretation becomes weak. A shorter protocol with clean monitoring often produces more useful information than a longer protocol with poor discipline.
Researchers often spend more time choosing a cycle length than building a handling system. That's backwards. If storage, preparation, and documentation are sloppy, the duration question becomes secondary because the data are already compromised.
TA-1 research requires routine laboratory discipline. Reconstitution practices, storage conditions, temperature control, and sterile handling all affect whether the material remains suitable for the protocol being run.

A few habits matter more than people think:
When researchers report that a peptide “didn't do much,” the failure is sometimes procedural rather than biological. Inconsistent preparation, weak recordkeeping, and poor timing can erase the signal a protocol was supposed to detect.
The research log should make the protocol reproducible for someone who wasn't in the room. If the record only says “TA-1 administered,” it isn't useful.
A strong log usually includes:
Documentation is part of the experiment. If it isn't written down clearly, it usually can't be defended or repeated.
This matters even more in peptide work because many protocols are iterative. Researchers often refine timing, frequency, or observation windows over successive runs. Clean records are what make those refinements meaningful.
The best answer to Thymosin Alpha 1 how long to take is that there isn't one default timeline. The literature supports everything from 5 to 7 day short courses to 6 to 12 month longer regimens, with intermediate structures in between. The deciding factor is the biological question.
That's the pattern behind the apparent inconsistency. Acute studies often use shorter windows because the endpoint is immediate. Chronic immune-focused research often runs longer because modulation needs time to emerge, stabilize, and be measured against predefined endpoints.
The practical lesson is straightforward. Don't copy a duration just because it appears often in the literature. Match duration to model, dose frequency to objective, and reassessment points to the kind of change you expect to see. Then document everything well enough that the protocol can be interpreted and repeated.
All information here is provided for educational and research purposes only. Thymosin Alpha-1 and related compounds should be treated strictly within lawful laboratory, analytical, and preclinical research frameworks. They are not presented here for human use, self-experimentation, or medical advice.
Researchers who need a dependable source of high-purity materials can explore Peptide Warehouse USA for laboratory and analytical peptide products supported by transparent batch documentation, third-party testing records, and a research-only supply model. Learn more about their catalog if you're comparing options for your next peptide study.



