No products in the cart.
You're likely here because you have a practical research decision to make. A needle-free PT-141 format sounds easier to work with, but ease of use isn't the same thing as predictable delivery. When researchers compare PT-141 nasal spray vs injection, the core question is not merely convenience. It's which route gives you the level of control, consistency, and risk management your study needs.
That decision matters more with peptides than many people expect. The active compound is the same, but the route changes absorption behavior, timing, handling demands, and the quality of the regulatory history behind the format. In a research setting, those differences affect protocol design, interpretation of outcomes, and how confidently you can compare one session to the next.
A useful comparison has to go beyond a casual pro-and-con list. It has to look at mechanism, pharmacokinetics, side effects, lab handling, and the historical reason injection became the benchmark while intranasal PT-141 remained outside formal approval pathways.
The cleanest way to think about this comparison is simple. Injection is usually the stronger route when you need repeatable exposure and tighter control. Nasal spray is often the lower-friction route when you value operational simplicity and can tolerate wider variability.
For research chemists, that trade-off shows up everywhere. It appears in onset windows, duration, side-effect patterns, local tolerability, and the amount of historical validation attached to each route. It also affects how much noise you introduce into your study design before the peptide itself has even had a chance to do anything.
Working rule: If your protocol depends on stable dose-to-dose performance, administration route is not a minor variable. It is part of the intervention.
PT-141, also known as bremelanotide, is a synthetic peptide derived from the melanocortin family. Pharmacologically, it's discussed as a melanocortin receptor agonist, particularly in relation to central receptors involved in arousal signaling. That central action is what makes the compound distinct from approaches built around peripheral vascular effects.

From a research perspective, the key point is that both nasal spray and injection use the same active peptide. You are not comparing two unrelated compounds. You are comparing two delivery systems for the same active agent.
That distinction keeps the analysis honest. If one route feels more reliable, that doesn't mean the molecule changed. It means the route changed how the molecule reached circulation and how consistently exposure occurred.
Researchers often jump straight to convenience. That's understandable, but it skips the most important baseline question. If the compound acts centrally, then the route's ability to deliver reproducible systemic exposure becomes a first-order variable.
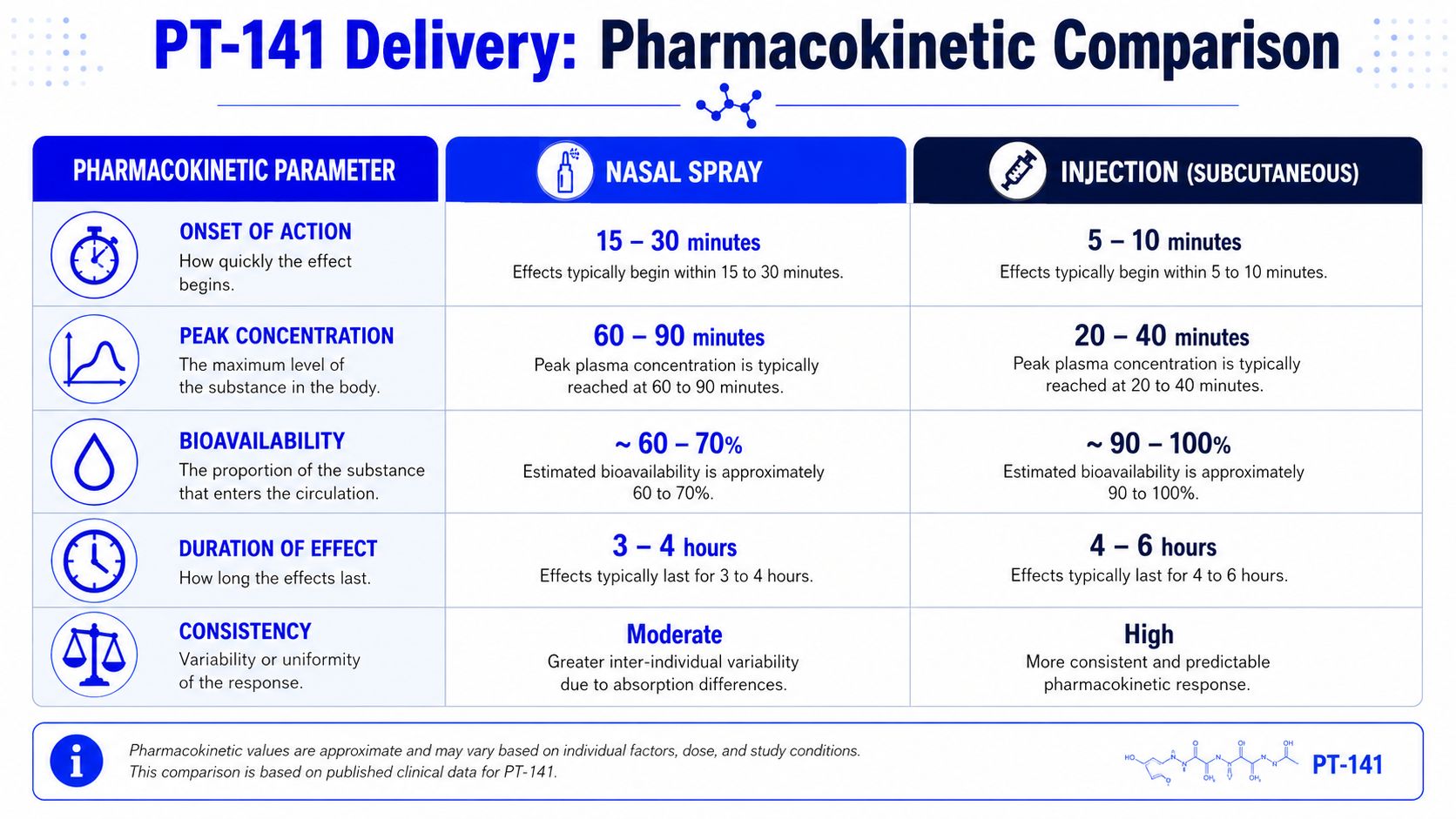
The most useful comparative framing is delivery efficiency. Intranasal use must cross the nasal mucosa, so absorption is more variable. Subcutaneous injection places the same active compound into fatty tissue and then into the bloodstream, which supports more stable plasma concentrations and more predictable dose-to-dose effects, as described in this PT-141 delivery comparison.
In practical lab terms, that means injection is usually the stronger benchmark when you care about consistency. Nasal spray remains relevant when you want a needle-free format or a lower-barrier administration route, but that convenience comes with more uncertainty around actual delivery.
A common study failure starts with an apparently simple assumption. Two groups receive the same peptide by different routes, the protocol keeps the nominal dose constant, and the team expects the exposure profile to be close enough for a clean comparison. With PT-141, that assumption can distort the readout before the first measurement is taken.
The practical question is not which route feels easier. The question is which route gives exposure characteristics that fit the study aim, while staying inside a defensible handling and risk framework. That is the difference between a convenience comparison and a usable pharmacokinetic comparison.
| Characteristic | Nasal Spray | Subcutaneous Injection |
|---|---|---|
| Delivery route | Across nasal mucosa | Into subcutaneous fatty tissue |
| Absorption pattern | More variable | More stable and predictable |
| Onset and duration | Faster initial uptake is often reported, with a shorter active window overall, as summarized in Boston Medical Group's comparison | Slightly slower onset is commonly reported, with a longer active window overall, as summarized in Boston Medical Group's comparison |
| Dose-to-dose consistency | Lower | Higher |
| Operational friction | Lower | Higher |
| Benchmark value for controlled study design | Moderate | Strong |
Intranasal delivery introduces more uncontrolled variables before the peptide ever reaches systemic circulation. Mucosal hydration, congestion, spray angle, residual runoff, and local irritation can all change how much material is retained and absorbed. In research terms, the labeled dose and the absorbed dose may diverge more often than teams expect.
Subcutaneous injection usually reduces that spread. It does not make PT-141 pharmacokinetics identical across subjects, but it removes several route-specific sources of noise and gives a cleaner basis for comparing timing, response magnitude, and repeatability across sessions.
That difference matters most in protocols built around narrow sampling windows.
If blood collection, behavioral observation, or physiologic monitoring has to occur at specific intervals, lower route variability usually matters more than administration convenience. This is the same logic used in any automation risk assessment guide. Control the avoidable sources of variation first, then interpret the signal that remains.
Reported timing summaries often make nasal spray look attractive because the onset can be earlier. That is useful if the protocol is testing rapid administration or shorter observation periods. It is less useful if the design depends on sustained exposure or repeated measurements across a broader window.
Injection usually fits the second case better. The active window is generally longer, which gives more room for scheduled assessments and lowers the chance that a late sample reflects declining exposure rather than a true biological difference.
Researchers should also keep the historical safety context in view here. Intranasal PT-141 was part of earlier development work, but the better characterized clinical route is subcutaneous administration. That does not automatically make injection the correct choice for every study. It does mean injection rests on a clearer record for exposure consistency and formal development history, while nasal delivery carries more uncertainty around real-world absorption performance.
Use nasal spray when the study is intentionally testing a lower-friction route, can tolerate wider exposure variability, and does not depend on a long effect window.
Use subcutaneous injection when the study needs tighter dose delivery, clearer timing interpretation, or stronger comparability across subjects and repeat administrations.
Use both routes only when route-dependent behavior is the actual research question. Otherwise, the added variability can complicate analysis without adding much scientific value.
A quick visual summary can help if you're comparing workflow fit with your team:
A common study problem appears after route selection, not before it. The protocol looks clean on paper, then adverse effects or route-specific tolerability issues start affecting repeat dosing, subject retention, and the interpretation of exposure-response data.
Subcutaneous PT-141 has the clearer documented adverse-event profile because it moved further through formal clinical development. One clinical summary reports nausea (40.0%), flushing (20.3%), injection-site reactions (13.2%), headache (11.3%), and vomiting (4.8%), along with a transient blood pressure increase of about 6 mmHg systolic and 3 mmHg diastolic, as outlined in this review of PT-141 for men. For a research team, that does not make injection unsafe by default. It means the expected liabilities are better mapped, easier to monitor prospectively, and easier to write into stopping rules and follow-up procedures.
Intranasal PT-141 often appears more tolerable in day-to-day use because it avoids needle-related reactions and may reduce the severity of some systemic effects. That practical advantage needs restraint in interpretation. The intranasal route also carries local tolerability concerns such as nasal irritation, and the historical development record is thinner. For study design, thinner history means more uncertainty around how administration quality, mucosal condition, and repeat-use irritation may alter real exposure across sessions.
That regulatory and historical context matters as much as the side-effect list. Injection has more burdensome reported adverse effects in many summaries, but it also rests on a better characterized safety package. Nasal delivery may look cleaner at first glance while still creating a harder analytical problem, because a subject can report fewer systemic symptoms and still receive less predictable drug exposure.
I treat those as different categories of risk. One is observed pharmacologic burden. The other is uncertainty burden.
For teams that formalize protocol hazards, a systems view helps. A peptide study carries compound risk, administration risk, documentation risk, and route-specific variability risk. A structured framework such as this automation risk assessment guide can help map how operational failures affect data quality, even when the immediate issue looks like tolerability rather than process control.
A practical safety readout is straightforward:
A common study failure starts at the bench, not in the assay readout. One session uses a carefully reconstituted injectable dose from a cold-chain vial. The next uses a nasal spray that was primed differently, stored inconsistently, or administered with a different technique. The label may show the same compound, but the handling variables are not equivalent.
That is why route selection should be written into the materials and methods section as an operational decision, not just a dosing decision. For PT-141, handling affects exposure consistency, sample integrity, and how defensible the protocol will look under later review.
Injectable PT-141 usually enters a lab as a vial format that requires controlled preparation. Staff should verify lot identity, concentration, storage history, and appearance before use. If reconstitution is required, the diluent, final concentration, timing, and storage window after mixing all need to be fixed in the protocol rather than left to technician preference.
Technique matters here. Peptides tolerate poor handling badly. Vigorous shaking can increase physical stress on the solution, so gentle swirling is the standard approach when a product calls for reconstitution. Use sterile tools, minimize unnecessary transfers, and document who prepared each dose and when.
Published summaries of the injection route describe a relatively standardized administration pattern, including timing before use and limits on dosing frequency, in this PT-141 dosing overview. In a research setting, the practical value of that history is procedural. Injection has been operationalized more consistently, which makes dose preparation and session-to-session replication easier to define.
Nasal PT-141 removes needles and often reduces prep time, but it shifts the control problem from reconstitution to delivery. Spray angle, priming, head position, residual volume in the device, and the condition of the nasal mucosa can all change how much compound reaches absorptive tissue.
Those variables are easy to underestimate. A nominally identical spray can produce different exposure if one session follows a strict administration script and another does not. Teams using this route should standardize priming steps, number of actuations, interval between sprays if applicable, device cleaning, and storage orientation.
Storage also deserves more attention than it usually gets. Multidose spray devices introduce repeated container handling and more opportunities for contamination, evaporation, or concentration drift if the formulation is not managed carefully. Injection vials have their own risks, but they are often easier to audit because the preparation chain is more explicit.
Some research groups source both formats from the same vendor, including Peptide Warehouse USA, to keep certificates, lot records, and purchasing documentation under one system. That does not make the two routes interchangeable. It only makes the comparison easier to document.
A few errors create avoidable variability in PT-141 work:
Good peptide work is usually decided by small controls applied consistently. With PT-141, handling discipline is part of the safety picture and part of the data-quality picture. That point matters even more here because the two routes do not carry the same development history or the same level of prior standardization.
A common study-design problem starts here. A team treats nasal PT-141 and injectable PT-141 as two packaging options for the same experiment, then writes one monitoring plan for both. That approach misses the main historical difference between the routes.
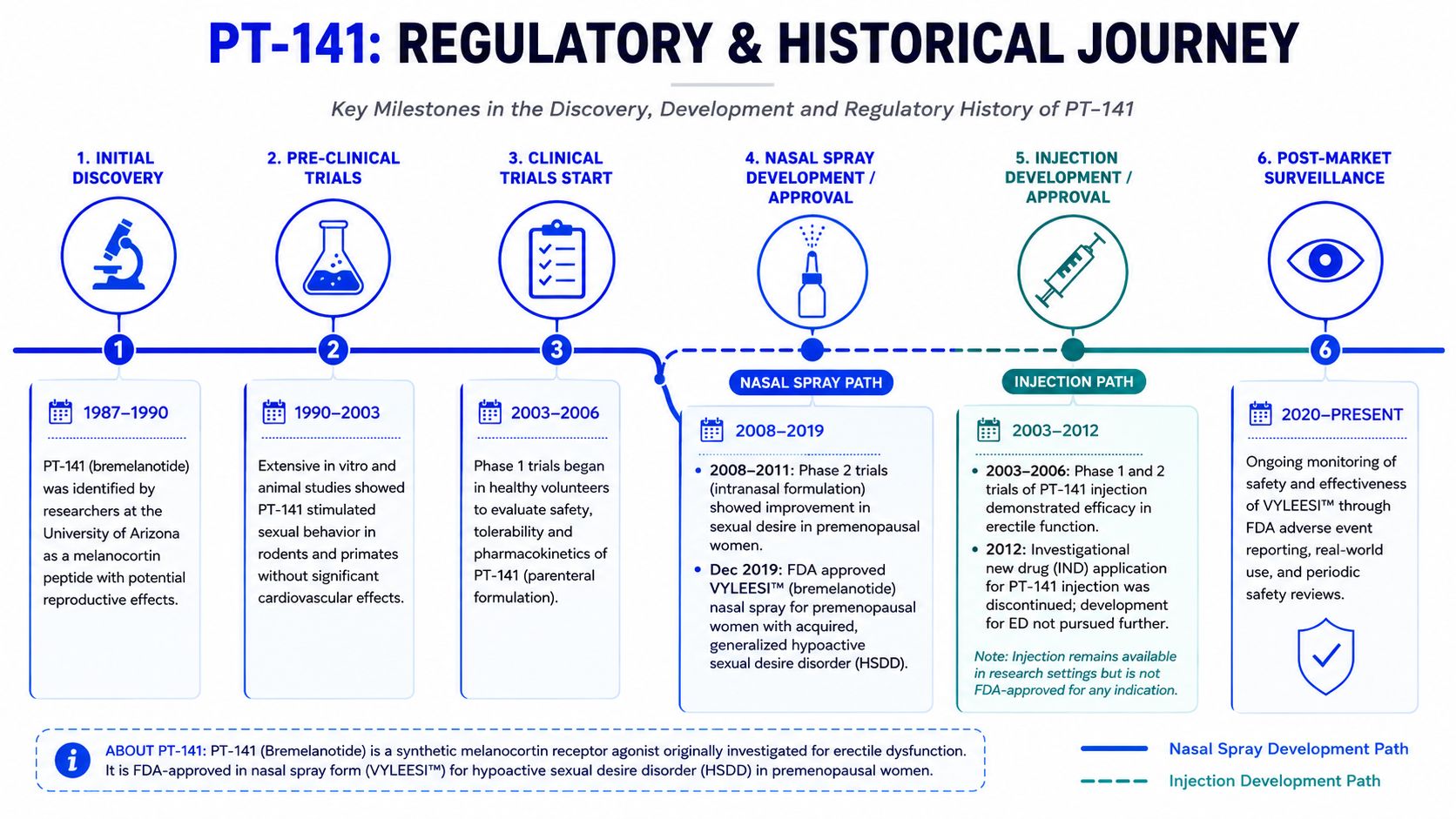
For bremelanotide, the clearest formal development path led to subcutaneous administration. The FDA approved the injectable product Vyleesi in 2019 for acquired, generalized hypoactive sexual desire disorder in premenopausal women, while no FDA-approved intranasal PT-141 product exists for men or women, according to this regulatory history summary.
For research work, that matters in practical terms. Injection has a defined regulatory precedent, published labeling history, and a clearer safety-monitoring model tied to a marketed route. It is still a compound that requires route-specific caution, but it is the better-established reference condition if the goal is controlled comparison or benchmark pharmacology.
Intranasal PT-141 sits in a different historical category. Earlier development work raised blood pressure concerns, and that history should shape how researchers write inclusion criteria, cardiovascular screening, and post-dose observation rules.
I would not describe nasal delivery as a simple convenience upgrade over injection. It changes absorption behavior, introduces route-dependent variability, and comes with a thinner formal development record. Those factors do not rule it out. They do mean the route belongs in exploratory protocols, not in casual equivalence claims.
A responsible comparison usually follows this hierarchy of confidence:
The main point is straightforward. Researchers are not only choosing between two administration methods. They are choosing between two very different development histories, and that difference should be visible in the protocol, the consent language, and the safety plan.
If your study needs the most stable reference model, injection is usually the cleaner choice. It offers more predictable dose-to-dose behavior, a longer working window, and the strongest formal development history attached to PT-141.
If your study is exploratory and route flexibility is part of the question, nasal spray still has value. It lowers administration friction and may align better with protocols focused on ease of use or shorter observation windows. The trade-off is that you accept more variability and a thinner regulatory record.
That's the core answer to PT-141 nasal spray vs injection. You are not choosing between “good” and “bad.” You are choosing between control and convenience, while also accounting for a meaningful difference in historical safety context.
For research teams, the right route is the one that matches the tolerance for uncertainty built into the protocol. If variability is a problem, injection is hard to beat. If route comparison itself is the subject, nasal spray belongs in the discussion, but only with the right compliance-aware framing and tighter procedural controls.
For labs comparing delivery formats, documentation standards, and peptide handling workflows, Peptide Warehouse USA offers PT-141 research products in both nasal spray and injectable formats for laboratory and analytical use. Learn more and explore options that fit your study design.



