No products in the cart.
Selective tissue repair sounds straightforward until you ask a harder question. Can you keep the protective biology of a molecule while removing the part that creates unwanted systemic effects?
That question sits at the center of interest in the ARA 290 peptide, also called cibinetide. It came out of erythropoietin research, but it wasn’t built to act like full erythropoietin. Researchers designed it to preserve tissue-protective signaling while avoiding red blood cell stimulation, which makes it unusually interesting for inflammation and neuropathy research.
For a lab scientist, that distinction matters as much as the headline claims. Mechanism affects study design. Early human data shape endpoint selection. Sourcing, purity, handling, and storage determine whether your results mean anything at all.
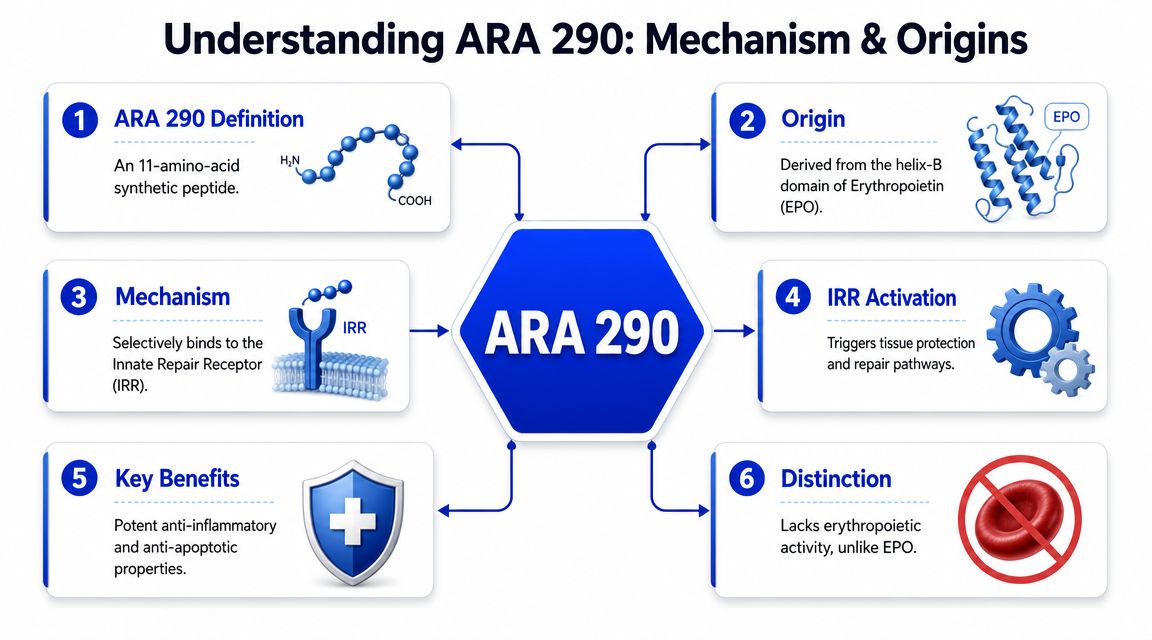
The ARA 290 peptide draws attention because it represents a precise design choice, not just another peptide added to a catalog. Researchers started with erythropoietin, identified the tissue-protective region of interest, and engineered a much smaller peptide intended to preserve repair signaling without the hematopoietic activity that would complicate chronic use.
That’s why the compound keeps showing up in discussions about small-fiber neuropathy, inflammatory signaling, and translational peptide research. The most useful questions aren’t hype-driven. They’re practical. What receptor does it target? What have human studies shown? Which endpoints look meaningful, and which claims still outrun the evidence?
For researchers, there’s also a second layer that often gets ignored. Even promising data are easy to misread if the peptide is poorly sourced, badly reconstituted, or handled without appropriate quality controls. ARA 290 is a good example of why research integrity starts before the first assay.
ARA 290 is best understood as a selective fragment strategy. It is an 11-amino-acid synthetic peptide engineered from the tissue-protective helix-B domain of erythropoietin, and published work describes it as acting through the innate repair receptor, often characterized as an EPOR/CD131 heteroreceptor, with anti-inflammatory and tissue-protective effects that occur without the red-blood-cell stimulation typical of EPO in this mechanistic review.
Full erythropoietin does more than one job. That’s useful in hematology, but it’s a problem if your research target is tissue protection rather than red blood cell production.
A simple analogy helps. Think of EPO as a multi-tool. If you only want the repair function, using the whole molecule means carrying along an extra function you may not want. ARA 290 was designed more like a dedicated instrument. It tries to isolate the repair-related signal.
That separation matters because it changes the risk-benefit logic in translational work. If a peptide can engage repair biology without stimulating hematopoiesis, it becomes more plausible to study in chronic inflammatory and neuropathic settings where erythropoietic activity would be undesirable.
Practical rule: When you evaluate ARA 290, don’t treat it as “small EPO.” Treat it as a deliberately narrowed signaling tool.
The receptor story is where many readers get tripped up. They hear “derived from EPO” and assume the biology should mirror EPO. It doesn’t.
The working concept in the literature is that ARA 290 preferentially engages the innate repair receptor rather than the classic erythropoietic pathway. That shifts the expected readouts. A researcher interested in this peptide should think first about inflammation-linked tissue stress, small-fiber function, and repair-associated endpoints, not blood-building outcomes.
In practical terms, that means your experiments should match the mechanism:
Researchers also care about what this mechanism does not justify. It doesn’t support broad claims about anti-aging, generalized regeneration, or universal healing. The peptide is interesting precisely because it is narrow, not because it is magical.
What should a careful researcher conclude when a peptide with a clean mechanistic story starts showing signal in human studies?
Early ARA 290 work matters because it moved beyond receptor theory into patients with neuropathic and inflammation-linked symptoms. The useful reading of that literature is narrow, indication-specific, and method-focused. For a lab trying to decide whether this compound belongs in a program, the key question is not whether the results sound promising. It is whether the endpoints, populations, and study design match the biology you plan to test.
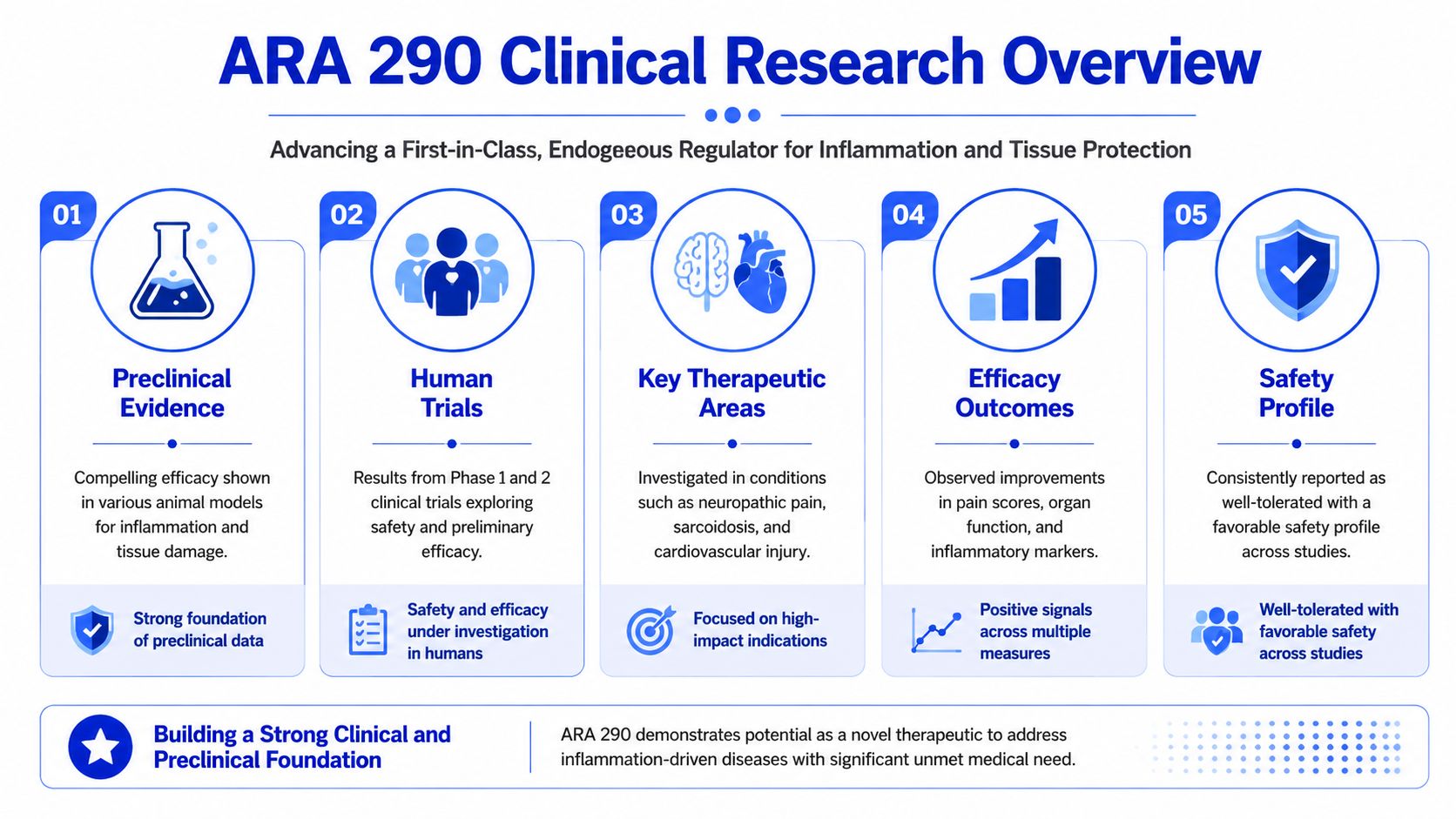
One of the clearer clinical datasets comes from type 2 diabetes with painful neuropathy. In a phase 2 study, investigators observed participants over a 56-day period and reported no potential safety issues. Over that interval, the ARA 290 group showed improvements in HbA1c, lipid measures, and neuropathic symptoms versus placebo. The study also tracked corneal nerve fiber density, and participants with low baseline CNFD showed a significant increase relative to placebo, as described in the Weill Cornell publication summary.
That combination is informative. Symptom scores can move for many reasons, including expectation effects or short-term changes in pain perception. Small-fiber structural measures give the dataset a different weight, because they ask whether the underlying tissue state may also be changing.
A separate clinical line studied sarcoidosis-associated small fiber neuropathy. In that trial, repeated dosing over 4 weeks produced a significant improvement in the Small Fiber Neuropathy Screening List score versus placebo, with a reported change of −11.5 ± 3.04 vs. −2.9 ± 3.34; p < 0.05. The same paper reported significant improvements in the SF-36 pain and physical functioning dimensions, and also stated that no abnormalities were seen in laboratory or clinical evaluations and no potentially drug-related adverse effects were reported in the published sarcoidosis study.
Preclinical findings tied to that same research program add context rather than proof. Investigators reported dose-dependent reductions in allodynia and suppression of the spinal microglia response. For experimental planning, that matters because it points toward inflammatory and neuroimmune pathways, not simple pain blocking. ARA 290 behaves less like a fast analgesic and more like a signal modulator that may alter the conditions driving neuropathic dysfunction.
The strongest published human signals cluster around neuropathic symptoms, fatigue, pain-related function, and small-fiber structure or function. They do not justify broad lifestyle or generalized regeneration claims.
The evidence is strongest when the question stays close to the studied populations and endpoints.
Across the early human literature, the recurring pattern is selectivity. Improvements appear in pain, fatigue, neuropathic symptom burden, and small-fiber-associated measures. That is different from a broad systemic effect claim. It suggests a researcher should build experiments around tissue stress, neuroinflammation, and small-fiber biology, then choose endpoints that can discriminate real biological change from temporary symptom fluctuation.
This is also where research integrity becomes practical. If a paper reports changes in CNFD, SFNSL, or other disease-linked measures, your own work should use assays and sample handling that can support the same level of specificity. Otherwise the translation breaks. The peptide may be sound, but the experiment becomes noisy.
The evidence base is still early-phase, short-duration, and indication-specific. Public discussions often move too quickly from mechanistic plausibility to therapeutic certainty. A more disciplined reading is that ARA 290 has a coherent rationale and encouraging human signals, but it still needs replication, careful endpoint selection, and tighter cross-study consistency. The PubMed overview discussing the small and early evidence base is useful on that point.
Researchers in oncology and translational medicine will recognize the pattern. A molecule can produce meaningful early data and still remain far from settled. That is why frameworks used in cancer clinical trials are relevant here too. Endpoint quality, patient selection, assay validity, and reproducibility determine whether an interesting signal holds up.
| Indication Studied | Key Endpoint(s) | Reported Outcome |
|---|---|---|
| Type 2 diabetes with painful neuropathy | HbA1c, lipid profiles, neuropathic symptoms, corneal nerve fiber density | Improved HbA1c and lipid profiles, significantly improved neuropathic symptoms versus placebo, and significant CNFD increase in participants with low initial CNFD |
| Sarcoidosis-associated small fiber neuropathy | SFNSL score, SF-36 pain, SF-36 physical functioning | Significant SFNSL improvement versus placebo, with reported changes of −11.5 ± 3.04 vs. −2.9 ± 3.34; significant improvements in pain and physical functioning |
| Early clinical literature across neuropathy-focused programs | Neuropathic symptoms, pain-related function, fatigue, small-fiber-associated measures | Signals are concentrated in neuropathy-relevant domains, with evidence that remains early-phase and indication-specific |
How much can a published ARA 290 dosing schedule tell you about your own experiment?
Less than many researchers hope, but more than skeptics sometimes admit. The useful signal is not a plug-and-play dose. It is the study logic behind the schedule, the route, and the timing of endpoint collection.
As noted earlier, the sarcoidosis-associated small fiber neuropathy trial used repeated dosing across a 4 week treatment window and reported improvement in symptom-focused outcomes relative to placebo. For a lab scientist, that matters because it frames ARA 290 as a compound studied through cumulative exposure over time, not as a one-time intervention expected to produce an immediate readout.
That distinction affects study design. If your hypothesis involves tissue protection, inflammatory signaling, or small-fiber remodeling, a single early measurement can miss the biology you are trying to detect. Peptide studies often fail for that reason. The compound is tested on the wrong clock.
A practical comparison helps here. Repeated-dose peptide work functions less like an anesthetic challenge and more like a cell culture differentiation protocol. The relevant question is often not, “Did anything happen in the next hour?” It is, “What changed after the system had enough exposure time to shift function or structure?”
Published human studies can help you set guardrails for experimental thinking:
That last point deserves more attention than it usually gets. Two labs can both report “the same dose” and still generate different exposure profiles because one used fresh solution, low-bind consumables, and verified concentration, while the other did not. For ARA 290, that kind of inconsistency can blur a real signal or create a false negative.
So the responsible use of the literature is straightforward. Borrow the experimental reasoning, then adapt it to your model with documented justification. Record why you chose the route, why your dosing interval matches the mechanism under study, and how you controlled pre-analytical variables before the peptide ever reached the assay.
Claims about a universal or standard ARA 290 dose sit outside what the early investigational literature supports. A better lab question is more specific. What exposure plan gives your experiment a fair chance to test the mechanism, while preserving traceability and reproducibility?
A peptide can have an elegant mechanism and promising literature, yet still produce worthless data if the vial content is inconsistent. That’s especially true with compounds like ARA 290, where researchers may be chasing subtle biological effects rather than crude binary outcomes.

Start with the Certificate of Analysis. If a supplier can’t provide batch-specific documentation, that’s the end of the conversation.
A useful COA review includes:
A second checkpoint is consistency across lots. One clean COA doesn’t solve the reproducibility problem if future batches drift. Good suppliers think in terms of batch control, not just one attractive PDF.
Low-quality peptide doesn’t just introduce noise. It changes the biology you think you’re observing.
If the sample contains degradation products, synthesis-related impurities, or inconsistent fill amounts, your assay may produce a false negative, a false positive, or an effect that can’t be replicated. In inflammation and neuropathy models, that problem gets worse because the expected signal may be nuanced.
A few practical warning signs show up again and again:
Good peptide science starts with skepticism. Verify the material first, then trust your assay.
For buyer awareness, that’s the key takeaway. The benefits of peptides in research depend on traceability, analytical support, and consistent manufacturing. Without those, even careful experimental design can collapse.
Bench technique matters more than many researchers admit. You can buy a strong peptide lot and still damage usability during reconstitution, storage, or repeated vial access.
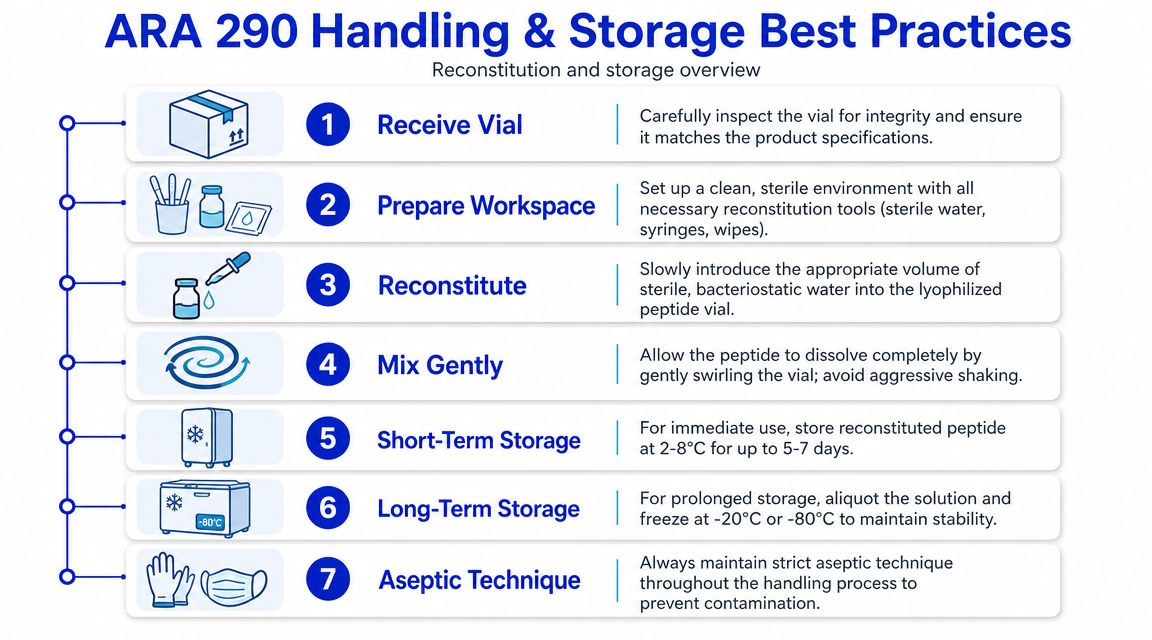
Treat reconstitution as a controlled procedure, not a casual prep step.
A short visual guide can help standardize staff handling across the lab.
Storage mistakes are usually boring, and that’s why they get overlooked. Repeated warming, light exposure, contamination during repeated puncture, and sloppy aliquoting can all degrade consistency.
A practical storage approach usually includes:
Small handling errors accumulate. If your endpoint is subtle, the storage workflow can decide whether the study succeeds.
The larger point is simple. Reconstitution and storage aren’t admin tasks. They’re part of the experiment.
How should a researcher read an encouraging safety profile without reading too much into it?
Start with scope. The published human data around ARA 290 are early-stage and indication-specific, so the right interpretation is narrow: studies have reported a generally favorable short-term tolerability picture in the populations examined, and the peptide has drawn attention in part because it was designed to separate tissue-protective signaling from the erythropoietic effects associated with full erythropoietin.
That design point matters, but it is not a safety guarantee. It is a hypothesis built into the molecule. Clinical studies then test whether that hypothesis holds under defined conditions, with specific inclusion criteria, dosing schedules, and monitoring plans. A lab reviewing ARA 290 should read safety findings the same way it reads efficacy findings. Ask what population was studied, how long exposure lasted, which adverse events were tracked, and whether the endpoints were strong enough to detect subtle problems.
This is also where research integrity becomes practical. “Research use only” is a regulatory boundary, but it is also a workflow standard. A responsible buyer should expect supplier documentation that matches that status: batch identity data, stated purity, storage guidance, and traceable records that support analytical work. If those basics are missing, the safety discussion is already on weak ground because you may not be studying the intended material with confidence.
ARA 290 is often grouped with peptides discussed in repair or inflammation-focused research, including BPC-157 and TB-500. That grouping can help at the level of broad interest, but it can also blur important differences.
A better comparison starts with mechanism. ARA 290 comes from an erythropoietin-derived tissue-protective region and is studied for signaling tied to the innate repair receptor. That gives it a more defined translational frame than the catch-all label of a “healing peptide.” In practice, that means a researcher should compare compounds by receptor biology, disease model, and endpoint fit, not by marketing category.
The lab analogy is simple. Putting these compounds in one bucket is like storing antibodies by box color instead of antigen specificity. It may be convenient, but it does not help experimental design.
For work centered on neuropathy models, inflammatory signaling, or small-fiber structure-function questions, ARA 290 has a mechanistic rationale that is easier to defend from the literature. For broader soft-tissue repair questions, a different compound may match the hypothesis more closely. The responsible choice is the one that fits the model, has the clearest sourcing and QC trail, and can be handled under conditions your lab can document and reproduce.
ARA 290 is one of the more interesting examples of targeted peptide design in translational research. It was built from an erythropoietin-derived tissue-protective region, but its relevance comes from what it avoids as much as from what it does. The peptide’s scientific appeal lies in selective repair-associated signaling without the erythropoietic activity that would complicate many chronic-use scenarios.
The published evidence is promising but narrow. Human studies support serious interest in neuropathy-related settings, especially where researchers care about symptom change alongside small-fiber structure or function. At the same time, the literature is still early-phase, short-duration, and specific to certain indications. That means careful endpoint selection and restrained interpretation aren’t optional.
For labs, the practical lesson is just as important as the biology. Good results depend on verified identity, defensible purity, batch traceability, disciplined reconstitution, and stable storage. The benefits of peptides in research only matter when the material quality and handling workflow are strong enough to support reproducible data.
Researchers who want reliable peptide inputs for laboratory and analytical work can learn more at Peptide Warehouse USA and explore high-purity options backed by batch documentation, COAs, and a research-use-only supply model.



