No products in the cart.
Individuals searching for ipamorelin peptide dosage often want a simple number. That’s understandable, but it misses the bigger issue. A dose only makes sense when you know what the peptide is trying to do, how often it’s being administered, and why timing changes the outcome of a research protocol.
Ipamorelin attracts attention because it’s commonly described as a selective growth hormone secretagogue with a cleaner endocrine profile than older compounds in the same category. That doesn’t remove the need for caution. It makes protocol design more important, not less. If you’re reviewing Ipamorelin peptide information, the useful question isn’t just “how much,” but “how should dose, schedule, handling, and monitoring fit together in a research-only setting?”
This guide treats dosage as part of a complete system. You’ll see how mechanism influences timing, how practical dosing ranges are usually framed, how reconstitution affects consistency, and why sourcing and documentation matter when reproducibility is the goal.
What does a useful ipamorelin peptide dosage look like in a research setting. It is rarely a single number written in isolation. A workable protocol connects dose amount, dosing interval, study aim, compound handling, and the expected behavior of a short-acting signaling peptide.
That distinction matters because ipamorelin is studied for its ability to trigger a receptor-mediated pulse, not for acting like a bulk replacement hormone. If researchers treat dosage as a static recipe, they can miss the reason one protocol produces a clean signal while another produces noise. The more useful question is not only “how much,” but “how much, how often, and why that schedule.”
A practical comparison helps here. Dose is the size of the knock on the door. Timing determines whether that knock arrives when the system can register it clearly, or whether repeated administration blurs the response. For peptides with short activity windows, schedule becomes part of the dose itself.
This is why responsible protocol design usually starts with four variables working together:
Researchers reviewing baseline Ipamorelin peptide information should treat it as a starting reference, not as a substitute for a study-specific protocol.
One mistake shows up repeatedly in peptide work. The nominal dose remains constant on paper, but inconsistent preparation or irregular administration changes effective exposure enough to distort the readout. In other words, two studies can list the same dose and still test meaningfully different conditions.
A careful ipamorelin dosage framework explains the logic behind the numbers before it assigns them. That approach improves interpretability, reduces unnecessary escalation, and keeps the work anchored in a research-only context where safety controls and documentation are part of the protocol, not an afterthought.
Ipamorelin is best understood as a signal peptide, not a bulk replacement compound. It’s commonly described as a selective agonist at the ghrelin or growth hormone secretagogue receptor, which means it acts more like a precise switch than a broad hormonal flood.
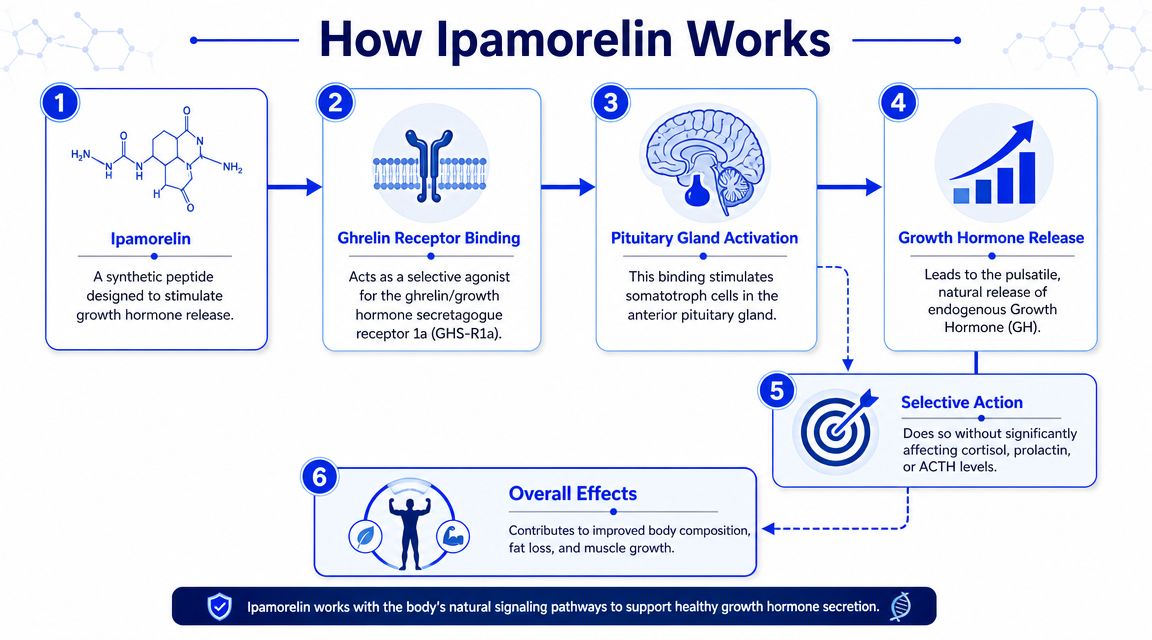
Think of receptor biology as a lock-and-key system. Many compounds fit imperfectly and turn several locks at once. Ipamorelin is discussed as interesting because it appears to engage the intended receptor pathway more selectively than older, broader secretagogues.
That selectivity matters in research for two reasons:
A practical way to frame it is this. If your study is asking whether pulsatile growth-hormone-related signaling affects recovery, body composition research endpoints, or tissue response, a more selective secretagogue is easier to work with than a noisier compound.
One of the clearest historical preclinical signals comes from a rat study indexed in PubMed. In that work, ipamorelin produced a dose-dependent increase in longitudinal bone growth rate from 42 microm/day in the vehicle group to 44, 50, and 52 microm/day in treatment groups, with P<0.0001 (PubMed record on dose-dependent bone growth effects).
That result doesn’t tell you how to run a modern lab protocol by itself. It does show that the compound’s biological activity was measurable at the tissue level in a controlled preclinical model.
A useful reading of the mechanism is simple: ipamorelin’s value isn’t that it “does everything,” but that it can produce a targeted signal that researchers can structure around.
For a lab technician, the takeaway is operational. The dose isn’t just a quantity in a vial. It’s a way to shape a receptor-mediated event. That’s why administration timing and consistency deserve as much attention as the listed micrograms.
Mechanism explains what receptor gets activated. Pharmacokinetics explains what happens after administration. That distinction is where many dosage discussions get blurry.
A peptide can have a useful target and still produce messy data if the exposure window doesn’t match the study design. With ipamorelin, researchers usually care less about “constant saturation” and more about how the timing of administration interacts with pulsatile signaling.
In practical protocol language, the real dose is a combination of amount, route, spacing, and consistency. If the peptide is administered once in a way that creates a short signaling event, that protocol is functionally different from the same total amount divided across separate administrations.
That’s why frequency often becomes part of protocol planning. A split schedule can be used when the goal is to distribute signaling opportunities rather than concentrate all exposure into a single administration window.
Consider two research mindsets:
Because this section doesn’t have verified numeric pharmacokinetic data to cite, the careful approach is qualitative. Researchers generally pay attention to the following:
The schedule should answer the study question. If the question is about repeated signaling, split administration may make more sense than a one-time daily exposure.
This is also where overcomplication hurts. A more intricate protocol isn’t automatically better. If staff cannot maintain identical preparation, timing, storage, and administration steps across study days, the protocol may add noise instead of insight.
This is the part most readers came for, but the numbers only make sense with the logic above in mind. Human-facing dosage guides repeatedly describe 200 to 300 micrograms per day as the most common ipamorelin range, usually by subcutaneous injection, and often split into 2 doses of 100 to 150 micrograms morning and evening. Beginner protocols are commonly listed at 100 to 150 micrograms once daily, while advanced protocols can go up to 400 micrograms per day (human-facing ipamorelin dosage guide).
| Protocol Level | Daily Dosage (mcg) | Administration Frequency |
|---|---|---|
| Beginner | 100 to 150 | Once daily |
| Common range | 200 to 300 | Often split into 2 doses |
| Advanced | Up to 400 | Divided schedule |
These ranges are useful as orientation points, not as universal instructions. A protocol should still reflect the study model, the schedule burden, and the monitoring plan.
A practical way to choose among these patterns is to match the protocol to the level of complexity your lab can execute.
The logic here isn’t unique to peptides. In emergency medicine training, dose discussions also make more sense when tied to route, indication, and timing rather than memorized in isolation. That’s why structured references like these lidocaine dose ACLS guidelines can be useful as a parallel example of how professionals connect dosing numbers to context.
Don’t choose a protocol because it looks “stronger.” Choose it because your handling process, sampling schedule, and study objective support it.
There’s also a common practical misunderstanding around split dosing. Splitting a daily total isn’t automatically about increasing total exposure. Often it’s about shaping the timing of the signal. If the objective is to evaluate repeated stimulation windows, dividing the administration can be more informative than raising the total amount.
For labs comparing protocols, a simple matrix often helps:
If you need a concrete product example, Peptide Warehouse USA lists a CJC-1295 (NO-DAC) + Ipamorelin Blend for research catalog purposes, which is relevant when protocol design involves combined peptide systems rather than ipamorelin alone. That doesn’t change the core principle. The dosage framework still has to match the study question.
A peptide protocol can look perfect on paper and still fail in execution. Reconstitution quality, sterile technique, and concentration control directly affect whether the intended dose is the dose that gets administered.

Lyophilized peptide handling should be deliberate and repeatable. The exact diluent volume you choose depends on the concentration your protocol needs, so the first task is calculation, not mixing.
A sound lab workflow usually includes the following:
Confirm vial identity and batch records
Check the label, lot information, and accompanying documentation before opening anything.
Calculate the target concentration
Decide what concentration will make the administration volume practical and easy to reproduce. Labs often choose a concentration that simplifies syringe reading and reduces math at the bench.
Add diluent carefully
Introduce the diluent gently against the vial wall rather than blasting directly onto the powder cake. The goal is to preserve peptide integrity during reconstitution.
Mix without shaking aggressively
Swirling is generally preferred over harsh agitation. Foaming and rough handling add unnecessary variability.
Bench note: The easiest concentration to remember isn’t always the best one. Choose the concentration that produces accurate, repeatable withdrawals with your actual lab tools.
Storage discipline matters too. Once reconstituted, the solution should be stored under the conditions specified by the supplier documentation and handled with a clear date-labeling system so the team doesn’t rely on memory.
The commonly described route in dosage guides is subcutaneous injection, and that matters because route changes can alter how a protocol behaves in practice. In a research workflow, route consistency is part of dose consistency.
Useful administration habits include:
A short procedural review can help teams stay aligned before running repeated administrations:
The biggest avoidable error in peptide handling is informal technique. If two technicians reconstitute, draw, or administer differently, your dataset may reflect workflow variation as much as peptide behavior. Good protocol design always includes bench-level standardization.
What should a careful research team watch for once an ipamorelin protocol is running? The answer is not a single side-effect list. It starts with understanding what the compound is designed to do, how long that signal lasts, and where protocol decisions can create avoidable risk.
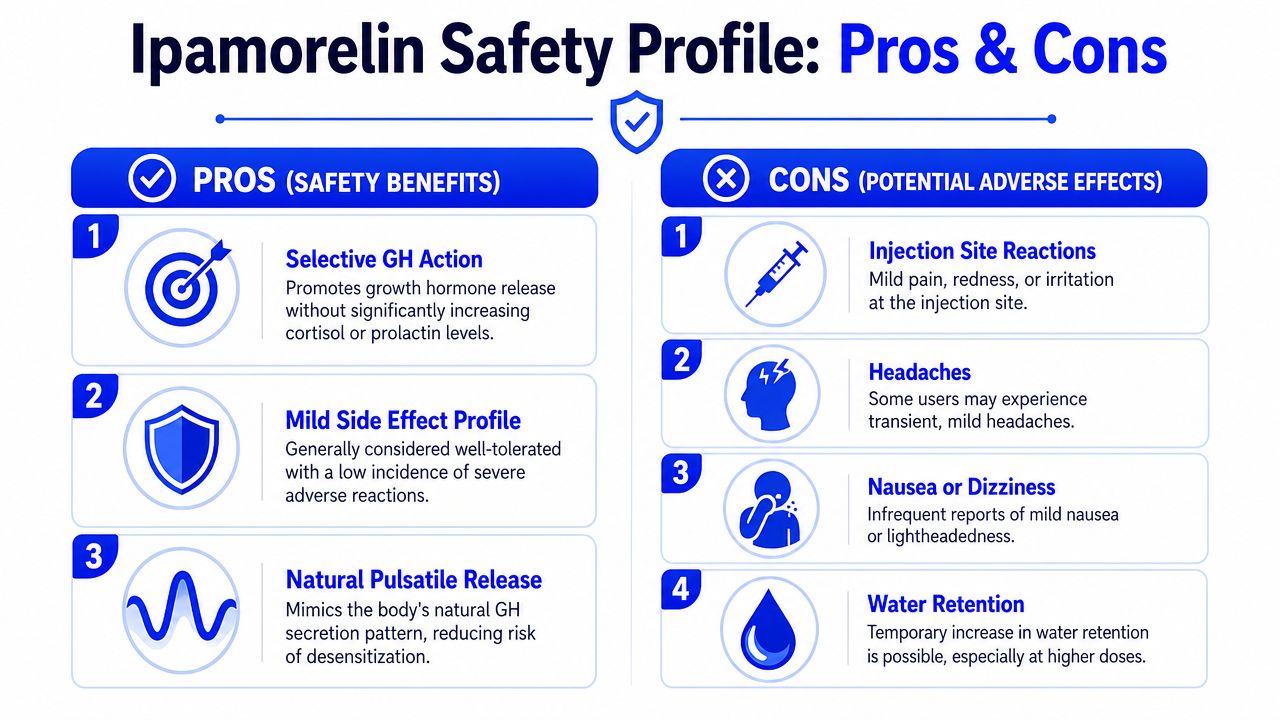
Ipamorelin is commonly described in research discussions as a selective growth hormone secretagogue acting through the ghrelin receptor pathway. That selectivity is the reason it is often viewed more favorably than older compounds in the same category. A narrower mechanism usually means fewer off-target signals to interpret.
Safety still depends on design quality.
A useful way to frame it is to compare protocol safety to signal-to-noise control in an assay. If the mechanism is fairly focused but the dosing schedule is poorly chosen, the observed effects may reflect protocol strain, cumulative exposure patterns, or handling inconsistencies rather than the peptide’s intended pharmacology. That is why adverse-effect review should stay tied to pharmacokinetics and dose timing, not just to a generic list of symptoms.
In research settings, the most practical concerns are often the least dramatic. Teams typically monitor for local injection-site reactions, short-term discomfort after administration, and changes that suggest the study schedule is producing a stronger or more persistent response than intended.
The key point is context. A finding that appears compound-related may come from concentration, injection technique, repeated site use, or an observation window that misses the expected pulse-like behavior of the peptide.
For that reason, monitoring should track both biological response and protocol execution.
Useful safety observations often include:
The “why” behind dosage matters most. Ipamorelin is generally used to produce a controlled secretagogue signal rather than constant receptor stimulation. If a protocol adds frequency or increases dose without a clear reason, the study may stop testing a clean pulse-based design and start testing accumulation of procedural stress.
That distinction matters because a more aggressive schedule can blur cause and effect. If irritation rises, or response patterns become less consistent, the problem may not be the peptide alone. It may be the interaction between dose size, dose spacing, route consistency, and study duration.
A restrained design often gives cleaner safety data.
Good safety practice in peptide research is mostly disciplined observation. It is less about dramatic intervention and more about preventing preventable noise.
A practical framework includes:
Selective pharmacology helps. Careful monitoring, conservative scheduling, and disciplined records are what make the safety profile interpretable.
The main lesson in ipamorelin dosage is simple. The number is only one part of the protocol. Mechanism tells you why the peptide is interesting. Scheduling determines how that signal is expressed. Reconstitution and administration determine whether the intended protocol is being delivered.
For that reason, research-only context matters. Ipamorelin should be approached as a laboratory compound used for analytical, preclinical, and related investigational purposes, not as a casual consumer product. If the source material is poorly characterized, the batch records are unclear, or the supporting documentation is thin, the dose printed on the label may not translate into reliable experimental input.
Sourcing standards should be strict:
The regulatory point is just as important. Research compounds need to stay within the boundaries of research use only. That protects the integrity of the work and keeps protocol decisions aligned with compliance expectations.
A careful researcher doesn’t just ask, “What’s the usual ipamorelin peptide dosage?” The better question is, “What dosage framework, schedule, and sourcing standard will give me interpretable results?”
If you’re comparing research suppliers and want documented peptide options for laboratory use, Peptide Warehouse USA offers a catalog built around batch testing, traceability, and research-use-only purchasing. Learn more and explore options that fit a controlled peptide research workflow.



