No products in the cart.
A vial of lyophilized peptide looks simple until you need to turn it into a usable solution without introducing error. That’s usually the moment people search for a peptide reconstitution calculator online. They want the math done fast, and they should. But the calculation is only one part of the job.
A clean reconstitution workflow starts earlier and ends later than most calculators admit. You need to understand what the powder is, choose an appropriate diluent, pick a reconstitution volume that supports accurate measurement, and handle the mixed solution in a way that protects stability. If any of those steps go wrong, neat arithmetic won’t rescue the result.
Reconstitution is the process of taking a lyophilized peptide, which arrives as a dry powder, and bringing it back into solution with a chosen diluent. That liquid form lets you measure the material accurately for laboratory, analytical, or preclinical work. Without that step, you can’t dose consistently.
The reason people look for a peptide reconstitution calculator online is straightforward. Manual math is easy to get wrong when you’re switching between milligrams, micrograms, milliliters, and syringe units. A calculator helps, but it only solves the arithmetic.
The complete protocol includes both numbers and technique. The concentration has to make sense for the measurement tool you’re using, and the handling has to protect the peptide after mixing. That’s where most low-value calculator pages stop too early.
A common bench failure starts the same way. A researcher has a lyophilized vial, picks an arbitrary diluent volume, gets a concentration that looks convenient, and only later realizes the syringe scale cannot measure the intended dose with enough precision. The math may still be correct. The setup is not.
Peptides are commonly supplied in lyophilized form, meaning the material has been freeze-dried into a powder to improve stability during storage and shipping. That dry state also leaves the final working concentration in the researcher’s hands, which is useful only if the concentration is chosen deliberately.
The vial is the starting material, not the finished preparation. Reconstitution sets the conditions for every draw that follows, including how accurately the solution can be measured, how easily the peptide dissolves, and how much handling stress the vial will see after it is opened.
Reconstitution creates a solution with a known concentration and a usable handling profile. Those are related, but they are not the same decision.
A highly concentrated vial can reduce injection volume, but it can also make small measuring errors more significant. A more dilute vial can be easier to measure on a fine syringe scale, but it increases the volume needed for each draw and may not suit the study design. Good reconstitution work balances dose precision, solvent compatibility, and expected vial use over time.
Practical rule: Do not draw from a vial until the concentration, intended dose per draw, and measuring device all match on paper.
That is why a peptide reconstitution calculator online should be treated as one tool in the workflow, not the workflow itself. The calculator can confirm arithmetic. It cannot decide whether the chosen concentration is realistic for your syringe markings, whether the diluent fits repeated vial access, or whether the peptide should be mixed gently and used within a narrower stability window.
For a peptide-specific example of how researchers often approach the physical mixing process and concentration planning together, see Weight Method’s semaglutide guide.
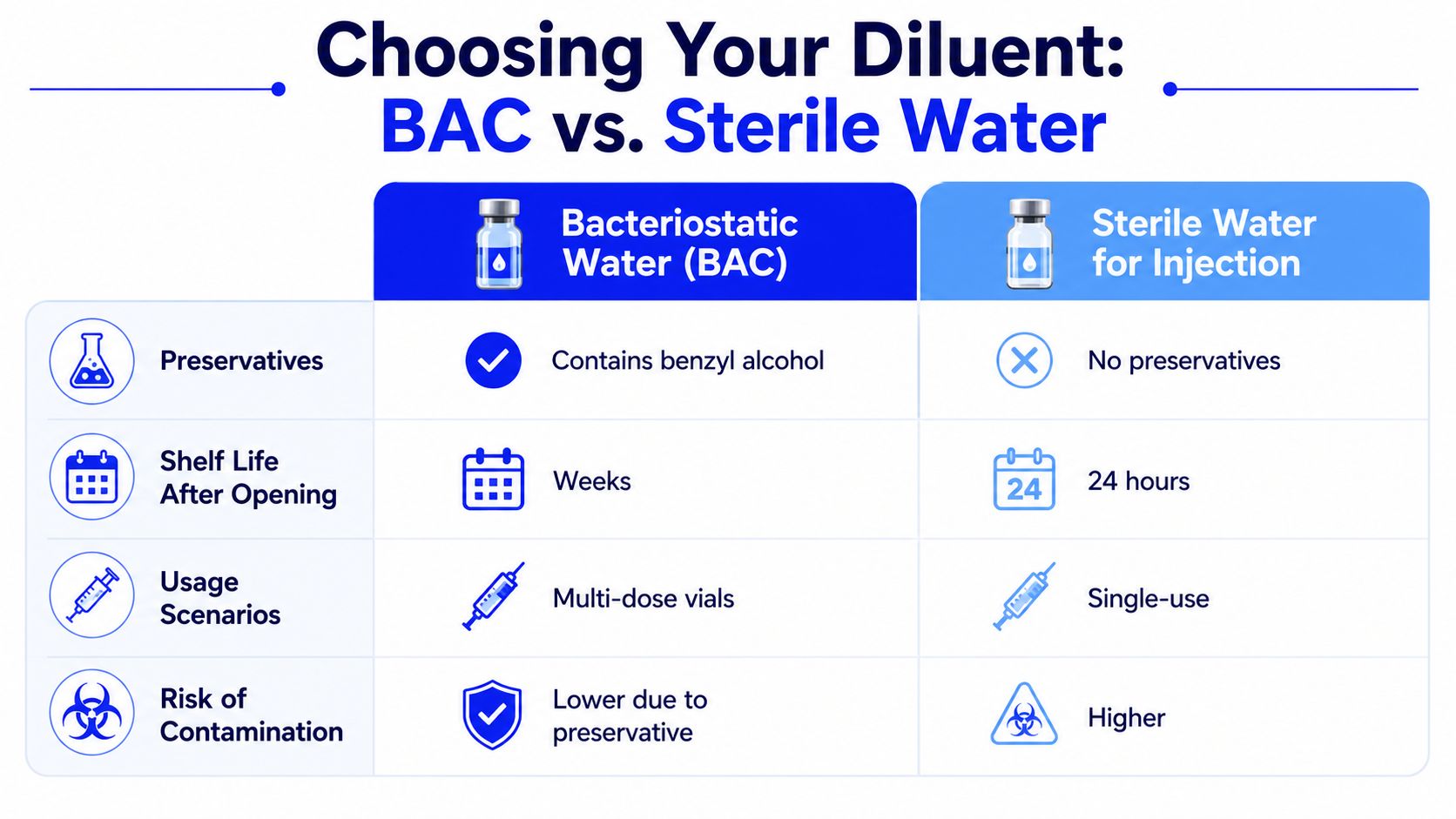
The first operational choice is usually the diluent. In many peptide workflows, that means selecting between bacteriostatic water and sterile water based on how the vial will be used after mixing, not based on habit.
| Diluent | Best fit | Main consideration |
|---|---|---|
| Bacteriostatic Water | Repeated vial access workflows | Includes a preservative |
| Sterile Water | Single-use or immediate-use workflows | No preservative |
That choice affects more than convenience. It changes how the vial is managed after reconstitution, how many times it may be accessed under the protocol, and how much risk is introduced during storage and repeated handling. Researchers who focus only on the final concentration often miss that point, and that is where otherwise correct calculations stop being useful in real lab work.
A common bench failure looks small at first. The math is correct, but the peptide was mixed with a diluent that does not fit the handling plan, the final concentration is awkward for the syringe on hand, and the vial label is incomplete. The result is avoidable variation in every draw that follows.
Diluent selection should be tied to how the vial will be used after reconstitution. If the protocol involves repeated vial access, many labs choose bacteriostatic water because the preservative supports that workflow. If the material will be prepared for immediate use or single-use handling, sterile water may be the better fit.
That decision affects storage, repeated needle entries, and how tightly the team needs to control the post-mix timeline. It also affects consistency across operators. A peptide reconstituted one way on Monday and another way on Thursday can produce different handling behavior even when the arithmetic is identical.
Write the diluent choice into the protocol, not just the notebook.
Reconstitution accuracy depends on ordinary supplies used correctly. Missing or substituting one item often leads to volume drift, contamination risk, or poor documentation.
Have these ready before the vial is opened:
Using one syringe for every step can save time, but it also increases the chance of misreading volume markings or carrying residue from one step into the next. Standardized supplies make the process easier to repeat and easier to audit.
Label the vial immediately after mixing. Memory is not a control measure.
The target concentration should be practical for the tools in use. That is the part many basic calculators ignore.
A highly concentrated vial may look efficient on paper, but very small draw volumes are harder to measure repeatably. Meniscus reading error matters more. Losses to the syringe wall, pipette tip, or vial surface matter more. A slight overdraw becomes a larger percentage of the intended dose.
A better working volume does four jobs at once:
This is the trade-off that deserves more attention. Higher concentration reduces injection volume, but it can also reduce dose precision if every withdrawal becomes a tiny fraction of a milliliter. In practice, the best reconstitution volume is the one that balances dose accuracy, handling ease, and the expected use period after mixing.
A common bench failure looks minor at first. The math is correct, the syringe is sterile, and the vial was mixed without visible residue. Then the planned dose works out to such a small draw that one inconsistent meniscus reading changes the result more than expected. Reconstitution succeeds on paper and fails in execution when the formula is treated as arithmetic instead of part of the protocol.
The first number to establish is the concentration after reconstitution.
Concentration = total peptide in vial ÷ total diluent added
That value sets every draw that follows. If it is wrong, every dose pulled from the vial is wrong in the same direction.
Use a fixed sequence:
Units are where avoidable mistakes happen. If the vial content is listed in milligrams and the intended dose is in micrograms, convert them before doing any dose math. The formula is simple. Unit inconsistency is what causes preventable dosing errors.
Once concentration is known, the withdrawal volume is straightforward.
Draw volume = desired dose ÷ concentration
This gives the liquid volume needed for one target dose. The number matters for more than convenience. It tells you whether the reconstitution plan is workable with the measuring device you have.
For example, a vial containing 5 mg of peptide reconstituted with 2 mL yields a concentration of 2.5 mg/mL. If the target dose is 250 mcg, convert that dose to 0.25 mg first. The draw volume is then 0.25 mg ÷ 2.5 mg/mL = 0.1 mL.
That is a usable result because it can be read clearly on many syringes. If the same vial were reconstituted into a much smaller volume, the required draw might become so small that routine handling error starts to matter more.
A correct formula can still produce a poor setup.
Very small draw volumes increase the effect of ordinary bench variation. Meniscus reading becomes less forgiving. Small droplets retained in the needle, syringe hub, pipette tip, or vial wall represent a larger fraction of the dose. Repeated withdrawals also become less consistent as the remaining volume falls.
This is the discipline simple calculators often miss. The right concentration is not the most concentrated solution possible. It is the concentration that gives a dose volume your team can measure repeatably, with the syringes or pipettes in use, over the full life of that reconstituted vial.
Manual calculation is still worth doing even if a calculator will handle the final numbers. It forces three checks that protect the protocol:
If any answer is no, revise the reconstitution volume before mixing. That saves time, reduces waste, and improves dose consistency across the whole study.
A common bench mistake starts before any diluent touches the vial. Someone enters the peptide amount correctly, picks an arbitrary reconstitution volume, accepts the first draw volume the calculator returns, and only then realizes the dose requires a withdrawal too small to measure cleanly with the syringe in hand. The calculator did its job. The setup was still poor.
Use a peptide reconstitution calculator online to test a plan before mixing, not to outsource judgment. A useful tool helps you confirm concentration, compare practical draw volumes, and catch unit errors before they become wasted material.
Online calculators usually ask for three values: total peptide in the vial, the volume of diluent to add, and the target dose per withdrawal. Enter each one from the label or protocol, not from memory.
Unit discipline matters here. Mg and mcg are easy to confuse, and a calculator cannot tell whether the wrong unit was typed with confidence. Verify the vial content first, then enter a proposed reconstitution volume, then check what draw volume corresponds to the intended dose.
If the tool offers unit switching or a syringe-style display, use it. Those features are helpful because they expose a practical problem early. A mathematically correct dose can still be a poor dosing setup if the withdrawal is difficult to read or reproduce.
Do not stop at the first answer.
Run one scenario, note the concentration and draw volume, then test a second reconstitution volume and compare the result. This takes less than a minute and often prevents an awkward setup that causes inconsistent withdrawals over the life of the vial.
A quick review should answer these questions:
| Check | Why it matters |
|---|---|
| Can the dose be measured cleanly with the syringe or pipette actually being used? | Small withdrawals increase reading error and retained-volume error |
| Does the concentration fit the study schedule? | The right setup should support the planned dose frequency without constant recalculation |
| Will repeated withdrawals remain workable as the vial empties? | Late-stage draws are often less consistent if the original setup was too concentrated |
That is how experienced lab staff use calculators. They compare workable concentrations, not just correct ones.
For a visual walkthrough of calculator thinking and reconstitution basics, this video is a useful companion:
The number on the screen only answers one question: what concentration results from a given vial amount and diluent volume. It does not tell you whether the chosen diluent suits the peptide, whether the material has fully dissolved, or how stable the solution will be after reconstitution.
Those decisions still control research quality. A calculator will not warn you that an aggressive concentration may dissolve slowly, that the selected diluent may be a poor fit for the peptide, or that repeated vial access can introduce handling variation after the math is done.
Use the calculator to set the concentration. Then verify the full process against the protocol: diluent choice, mixing method, achievable dose volume, labeling, storage conditions, and expected use period. That full-process approach protects dose accuracy better than calculator output alone.
A peptide can be mathematically correct and still be unusable at the bench. I have seen reconstituted vials fail for ordinary reasons: incomplete dissolution, contaminated stoppers, repeated warm-up cycles, and concentrations that looked efficient on paper but made accurate withdrawals harder in practice.
The first minutes after adding diluent matter more than many teams expect. Let the liquid run down the inside wall of the vial if possible. Hitting the powder cake directly can compact material against the glass or create foaming, which slows inspection and makes it harder to judge whether the peptide is fully in solution.
Use a slow swirl or gentle rolling motion. Do not shake aggressively. Rough mixing can introduce bubbles and can leave you guessing whether you are seeing foam, particulates, or undissolved material.
Do not draw from the vial until the solution looks uniform.
If the peptide is slow to dissolve, patience is usually better than force. Give it time, inspect against the light, and verify that no film or visible particles remain on the base or sidewall. A clear concentration target means little if part of the peptide is still stuck in the vial.
Post-reconstitution handling should be treated as part of dose control. Every stopper puncture, every tool change, and every extra minute at room temperature adds another chance for error.
A clean routine helps keep the sample consistent:
These steps protect more than sterility. They also reduce drift between early and late withdrawals, which matters when the study depends on repeatable dose volumes.
Storage conditions should match the peptide and the planned use period. The practical questions are straightforward. Will the peptide remain stable in the chosen diluent? How many times will the vial be accessed? Will the vial be refrigerated between uses, or frozen for longer-term storage under the protocol?
Temperature cycling is a common source of avoidable variation. Repeated warming and cooling can shorten usable life, especially after the peptide is already in solution. If the protocol allows aliquoting, that often reduces repeated vial access and limits stress on the main stock.
Label the vial clearly and immediately. Include concentration, diluent, preparation date, and storage condition. In shared lab settings, unlabeled or partially labeled reconstituted peptides create preventable risk.
The calculator gives you a concentration. Good handling preserves it.
A peptide reconstitution calculator online is useful for one reason. It makes the math fast and readable. That’s important, but it’s not the whole job.
Reliable reconstitution is a full-process discipline. You need the right diluent for the workflow, a reconstitution volume that supports accurate measurement, clean bench technique during mixing, and storage habits that protect the material after it goes into solution. When researchers get those pieces right, their calculations become meaningful because the liquid in the vial still reflects what they intended to prepare.
If you’re evaluating peptide sourcing and want materials backed by transparent documentation for research use, start with the same standard you’d apply to your protocol. Precision should begin before the vial is opened.
For researchers who want dependable sourcing to match careful bench practice, Peptide Warehouse USA offers high-purity research peptides with third-party documentation, including COAs and related batch records. Learn more, explore options, and build your workflow on materials designed for laboratory and analytical use.



