No products in the cart.

You’re probably here because your team keeps seeing the same pattern. Standard thyroid markers explain part of the biology, but not all of it. Autoimmune activity, tissue remodeling, receptor signaling, and metabolic cross-talk don’t fit neatly into a single TSH value, so the question becomes whether peptides for thyroid research can offer more precise experimental tools.
That question matters now because peptide science is no longer a fringe category. It sits inside a mature pharmaceutical and regulatory environment, yet thyroid-focused peptide work still has large mechanistic gaps. For a lab manager or translational researcher, that creates a useful tension. The platform is credible, but many thyroid applications remain open for careful preclinical design.
Most thyroid discussions stay at the symptom or hormone-replacement level. Research on peptides for thyroid function asks a different question. Instead of only replacing output, can a peptide influence the signaling network that determines output, immune targeting, or tissue response?
That distinction matters because the thyroid isn’t an isolated gland. It sits inside a layered endocrine system, receives upstream instructions, and in autoimmune states becomes a target of antibody-driven disruption. A peptide can therefore be relevant even if it doesn’t act directly on thyroid cells. It may alter receptor binding, immune signaling, neuroendocrine communication, or downstream tissue remodeling.
Peptide therapeutics also have stronger scientific footing than many people assume. In Paloma Health’s review of peptide therapeutics, the FDA approved 10 peptide drugs in 2021, the highest annual total on record at that time, compared with 6 in 2017, and by 2022 peptides accounted for 21.5% of all FDA-approved drugs. The same review notes major GLP-1 analogue sales, including Trulicity at $4.39 billion, Victoza at $3.29 billion, and Rybelsus at $1.68 billion, which shows peptide medicines are established therapeutic platforms rather than niche curiosities.
For thyroid research, that doesn’t mean any given peptide is validated for thyroid modulation. It means peptide chemistry, manufacturing, and translational development already have a credible path. That lowers the barrier for serious endocrine research while raising the standard for study design.
A lot of confusion comes from mixing very different peptide categories together:
Working rule: Don’t group all thyroid-relevant peptides into one bucket. Start by asking which layer of thyroid biology your experiment is trying to perturb.
The thyroid system makes more sense if you think of it as a command chain with feedback. One structure sends instructions, the next relays them, and the gland at the end produces hormones that report back to the system. If you skip that architecture, peptide experiments become hard to interpret.
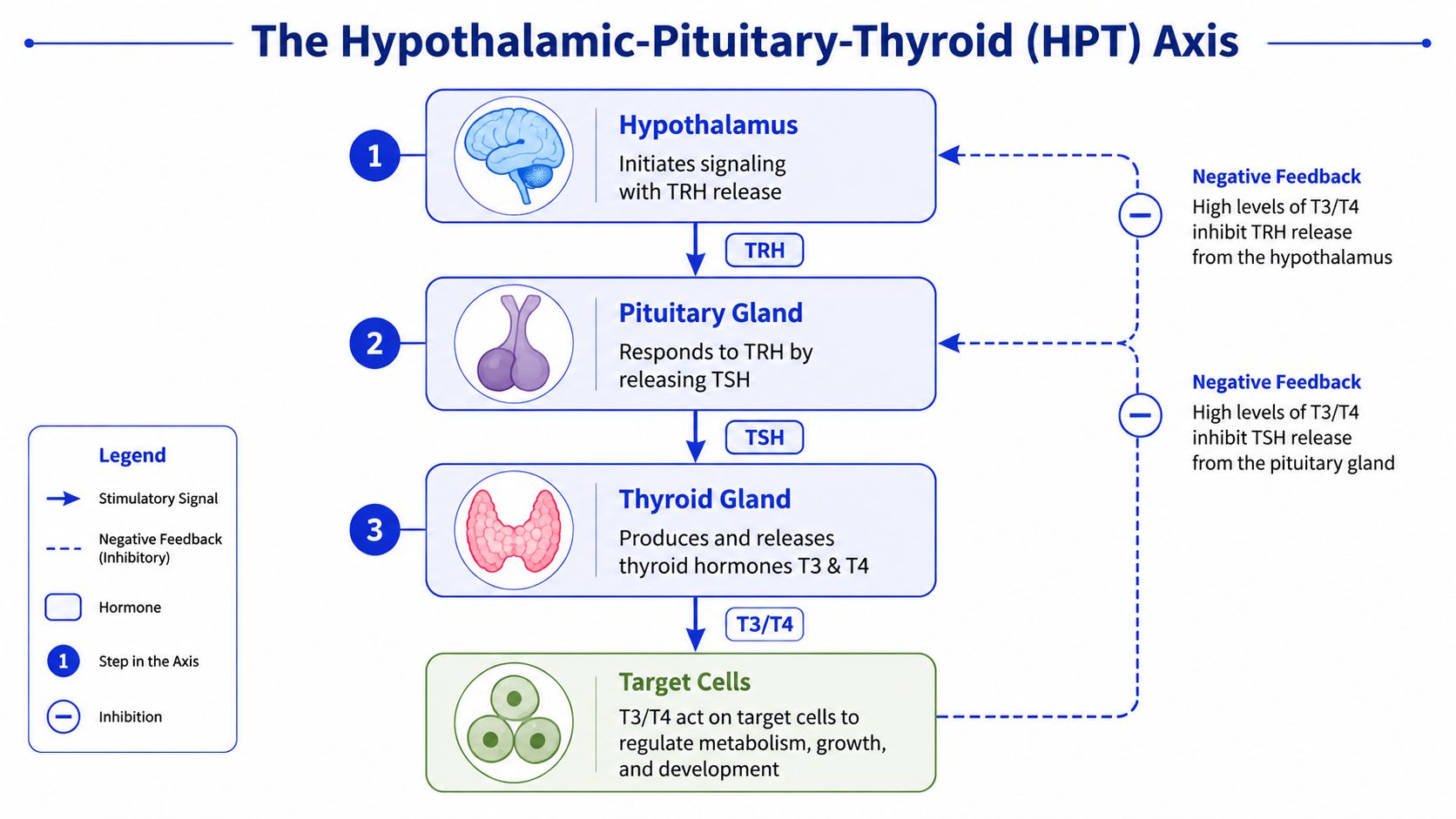
At the top sits the hypothalamus, which releases thyrotropin-releasing hormone, or TRH. TRH signals the pituitary gland to release thyroid-stimulating hormone, or TSH. TSH then acts on the thyroid gland, which produces thyroid hormones, mainly T4 and T3.
A thermostat is the simplest analogy. The hypothalamus senses the broader state of the organism and issues an initial signal. The pituitary acts like the relay controller, and the thyroid is the device that changes output.
The feedback is what keeps the system stable. When circulating thyroid hormone levels rise, they suppress further TRH and TSH signaling. When they fall, the system ramps back up. That negative feedback loop is why a change at one node can produce delayed or apparently contradictory effects at another.
If a peptide changes TSH, that doesn’t automatically tell you whether it acted at the hypothalamus, pituitary, or thyroid. The same measured endpoint can emerge from different mechanisms. A lab that only measures one hormone may miss the actual site of action.
That’s especially important when you’re evaluating compounds discussed under the umbrella of peptides for thyroid support. Some candidates may influence central signaling. Others may affect peripheral hormone handling, tissue inflammation, or receptor-level immune interactions.
Consider three common interpretation errors:
Use the axis map before you choose assays. If the peptide’s proposed mechanism is upstream, downstream-only readouts can blur the signal.
A useful way to organize peptides for thyroid research is by pathway, not by brand or popularity. That keeps the biology clear. It also prevents the common mistake of comparing compounds that operate on completely different levels of the system.

The most straightforward category includes peptides that affect the hypothalamic-pituitary-thyroid axis directly. TRH and TRH analogs are the classic conceptual example. In research terms, these compounds are valuable because they probe whether the limiting step sits in central endocrine signaling rather than in the thyroid gland itself.
A related but distinct class includes TSH receptor-directed peptides. These don’t merely increase signaling globally. They can be engineered to interact with the receptor biology that defines how thyroid tissue responds to stimulation or immune attack.
That receptor-directed logic becomes much more interesting in autoimmune disease models, especially Graves’ disease. In a study published in Endocrinology on peptide 836, a thyroid-targeted cyclic peptide reduced thyroid hyperplasia and histological damage in a long-term mouse model of Graves’ disease, and high T4 levels returned to normal starting 15 weeks after peptide therapy began. That result is notable because it points to a disease-modifying, receptor-based immunomodulatory effect rather than a simple symptomatic shift.
Autoimmune thyroid disease creates a different research problem from hormone deficiency alone. In Graves’ disease and Hashimoto’s-related settings, the relevant question often isn’t just hormone output. It’s whether a peptide can alter the immune behavior that keeps driving gland dysfunction.
That’s where cyclic peptides aimed at the TSH receptor stand out. Their value isn’t that they’re “thyroid peptides” in a generic sense. Their value is that they can be designed around a known antigenic or receptor-interacting structure.
Researchers can think about this class through several endpoints:
A peptide that changes autoantibody behavior is doing a very different job from one that simply perturbs TSH release.
Some peptides may influence thyroid-relevant biology without acting as primary thyroid ligands. Consequently, readers often get confused, as indirect pathways can still matter experimentally.
Metabolic peptides may alter energy balance, inflammatory tone, or hormone sensitivity in ways that affect thyroid readouts. Cellular-support peptides are discussed even more broadly, often in relation to repair or oxidative stress. Those categories are worth studying, but they demand tighter mechanistic controls. If a peptide changes body weight, feeding behavior, or inflammation, any thyroid signal may be secondary.
There’s also an unresolved mechanistic area around bioregulator peptides and epigenetic claims in thyroid-related settings. The main takeaway for a serious lab is restraint. These hypotheses may be worth exploring, but they need direct molecular mapping before they should be treated as established thyroid mechanisms.
A common study-design problem looks like this. A team sees a peptide discussed in endocrine circles, adds it to a thyroid protocol, and then struggles to explain whether any signal came from the thyroid axis, the immune system, or a broader stress or repair pathway. In thyroid research, that distinction is the whole experiment.
For that reason, the compounds below are easier to evaluate if you sort them by mechanism first and name second. A peptide that acts upstream at the hypothalamic-pituitary-thyroid axis answers a different question from a peptide that shifts TSH receptor-directed immunity in a Graves’ model. The practical goal is not to build a shopping list. It is to build a mechanistic map that helps a lab choose the right model, controls, and readouts.
| Peptide | Proposed Mechanism of Action | Primary Research Area |
|---|---|---|
| TRH | Direct stimulation within the HPT axis, upstream of TSH release | Axis signaling research |
| Protirelin | TRH analog used to study pituitary-thyroid responsiveness | Diagnostic and endocrine signaling research |
| Peptide 836 | TSH receptor-directed cyclic peptide with immunomodulatory activity in Graves’ model | Autoimmune hyperthyroidism research |
| P19 | Cyclic peptide that improved thyroid function, shifted anti-TSHR antibody subpopulations, and improved orbital tissue markers in Graves’ model | Graves’ disease and thyroid eye disease research |
| Selank | Neuroimmune and stress-axis peptide often considered in HPA-HPT cross-talk discussions | Neuroendocrine and immune interaction research |
| Semax | Central nervous system peptide relevant to stress-response and neuroendocrine signaling contexts | Neuroendocrine research |
| BPC-157 | Commonly discussed in repair and gut-barrier contexts, with thyroid relevance remaining indirect and protocol gaps still unresolved | Regenerative and autoimmune-adjacent research |
| TB-500 | Tissue repair-oriented peptide of interest where systemic healing or inflammatory context may intersect with endocrine models | Regenerative research |
| Thyrogen | Recombinant TSH analog used in thyroid-related diagnostic settings | Clinical analog and thyroid stimulation research |
| Thymosin Alpha-1 | Immune-modulating peptide relevant to studies of immune balance in autoimmune contexts | Immunology and autoimmune research |
The cleanest way to read this table is to group the entries into three experimental buckets.
First are axis probes such as TRH, protirelin, and recombinant TSH analogs. These are useful when the lab wants to test responsiveness within the signaling chain itself. They function like stimulus reagents in a circuit test. If the question is whether the pituitary or thyroid responds appropriately to upstream input, these compounds fit.
Second are immune-focused peptides such as Peptide 836 and P19. These belong to a different framework. Instead of asking whether the gland can respond to endocrine stimulation, they ask whether receptor-directed autoimmunity can be reshaped in a way that changes thyroid output and tissue pathology at the same time.
That distinction matters.
One of the more informative examples is P19. In the PubMed-indexed Graves’ disease study on P19, investigators reported improvement in thyroid function together with changes in anti-TSHR antibody subpopulations and orbital tissue markers. For a research team, that pattern is useful because it links mechanism across levels of biology. Serum output changed, but so did the immune profile and a disease-relevant peripheral tissue compartment. That is a stronger experimental signal than a hormone shift alone.
A third bucket includes peptides discussed because they may alter context rather than primary thyroid signaling. Selank and Semax are usually considered through neuroendocrine or stress-response pathways. BPC-157 and TB-500 are more often placed in repair, inflammation, or barrier-function discussions. These compounds may still be relevant in thyroid-adjacent experiments, but the hypothesis has to be framed carefully. If body weight, feeding behavior, inflammatory tone, or stress signaling changes first, the thyroid readout may be downstream of that broader shift.
Match the peptide class to the biological question.
A useful analogy is assay interference versus assay signal. If a peptide changes several systems at once, the thyroid phenotype can look important while still being secondary. That does not make the result uninformative. It means the study needs stronger controls, clearer timing, and a mechanism-specific interpretation.
For labs screening candidates, the table works best as a triage tool. It helps identify what kind of experiment a peptide belongs in, what confounders need attention, and whether the expected effect should appear at the level of hormone release, receptor immunology, or broader organismal physiology.
A thyroid peptide study fails most often at the design stage, not the assay stage. Teams choose a peptide first, then build endpoints around whatever is convenient to measure. The better sequence is the reverse. Start with the mechanism you think you’re testing, then choose endpoints that can falsify that mechanism.

For most thyroid-focused preclinical work, a basic serum panel should include TSH, T4, and T3. In autoimmune models, that isn’t enough. You’ll also want antibody-focused measures that align with the model you’re using, along with tissue-level assessment of the thyroid itself.
A practical endpoint stack often includes:
These layers matter because hormone normalization can hide ongoing tissue pathology. The reverse is also true. An immune-active peptide may improve gland histology before downstream serum patterns stabilize.
Experimental caution: If your peptide is supposed to be immunomodulatory, don’t let a normal TSH value convince you the mechanism worked. Check the tissue and antibody biology.
A clean way to think about study design is to group experiments by biological question.
One design asks whether the peptide affects the axis directly. In that case, use a model where central endocrine signaling can be observed without overwhelming autoimmune noise.
A second design asks whether the peptide changes autoimmune targeting. That’s where Graves’-type models, receptor-directed peptides, antibody subfraction analysis, and histopathology become more informative than serum hormones alone.
A third design asks whether a peptide combination changes repair or immune resilience in autoimmune thyroid settings. The literature on this particular aspect is notably thin. In this discussion of LDN and peptide protocol gaps in Hashimoto’s-related contexts, a significant research gap is identified around data-driven protocols combining peptides such as BPC-157 with Low-Dose Naltrexone. The problem isn’t lack of interest. It’s lack of controlled studies defining dosing structure, sequencing, or consistent outcome tracking such as antibody reduction.
A useful benchmark for those combination studies would be a multi-layer design that includes:
A short overview of experimental thinking can help teams align on setup before committing resources:
In peptide work, quality control isn’t a purchasing detail. It’s part of the experimental system. If identity, purity, endotoxin status, or batch consistency are uncertain, you can’t confidently assign the biological effect to the sequence you intended to study.
For thyroid research, this point becomes more important because many relevant endpoints are subtle. Small changes in hormone patterns, antibody profiles, or histology can be easy to misread if the input material varies across lots.
A responsible sourcing checklist should include:
This is not optional. The more mechanistic your study is, the more a low-quality material can create false positives or wash out a real signal.
Thyroid safety concerns often come up in peptide-adjacent discussions because GLP-1 receptor agonists are highly visible endocrine drugs. The key point is to separate proven human risk from early noise or surveillance artifacts.
In Mayo Clinic’s report on a real-world GLP-1 receptor agonist study, researchers followed 41,112 patients who started a GLP-1 receptor agonist. The absolute risk of thyroid cancer was 0.17%, and the overall hazard ratio was 1.24 with a 95% confidence interval of 0.88 to 1.76, which was not statistically significant. There was a temporary increase in diagnoses during the first 12 months with a hazard ratio of 1.85 and 95% confidence interval of 1.11 to 3.08, but that association disappeared after year one, supporting detection bias rather than a proven causal cancer signal.
That doesn’t validate unrelated peptides. It does provide useful context. Human thyroid safety questions around peptide-based endocrine agents should be assessed with cohort data and mechanism, not rumor.
In a research setting, the right response to a safety signal is tighter classification. Ask whether the concern is sequence-specific, class-specific, model-specific, or a surveillance artifact.
A lab team has a reproducible thyroid phenotype in hand, but the mechanism is still blurred. Is the signal coming from central axis regulation, receptor-level effects in thyroid tissue, immune activity around the gland, or a secondary metabolic shift? Peptide research is useful here because it lets investigators narrow the question before they scale the model.
That narrower framing is a primary opportunity in thyroid science. Broad endocrine interventions can change several systems at once, which makes interpretation harder. Peptides can work more like targeted probes. In practical terms, they help a research group test whether a response belongs to the hypothalamic-pituitary-thyroid axis, a thyroid receptor pathway, an autoimmune process, or a repair program acting outside direct hormone control.
The most informative studies pair the peptide class with the biological question from the start. Receptor-directed cyclic peptides fit experiments centered on Graves’ disease mechanisms. Axis-active peptides fit studies focused on upstream endocrine regulation. Peptides associated with tissue repair or immune signaling can still matter, but the design has to separate indirect improvement from genuine thyroid modulation.
Study infrastructure will decide how useful the next wave of findings becomes. Combination protocols in autoimmune thyroid models need controlled comparisons rather than informal stacking. Claims about epigenetic or mitochondrial effects need direct readouts, time-course mapping, and tissue-specific interpretation. Reproducibility also starts before dosing, with clear identity testing, purity data, storage controls, and lot-level documentation.
For teams building thyroid-focused preclinical workflows, that is the productive tension in this field. There is enough mechanistic rationale to justify careful experimentation, and enough uncertainty to reward disciplined study design.
If your group is sourcing compounds for laboratory or preclinical work, Peptide Warehouse USA offers research-use-only peptides and related compounds with batch documentation, COAs, and analytical support materials. Review their materials if your team needs traceable inputs for thyroid-related peptide studies.



