No products in the cart.

Most articles about PT-141 nasal spray treat the nasal route as the simple option. For research work, that’s often the wrong starting point. Convenience is real, but convenience can hide the variables that matter most: absorption, formulation stability, bottle-to-bottle consistency, and whether a “spray dose” behaves like the label suggests.
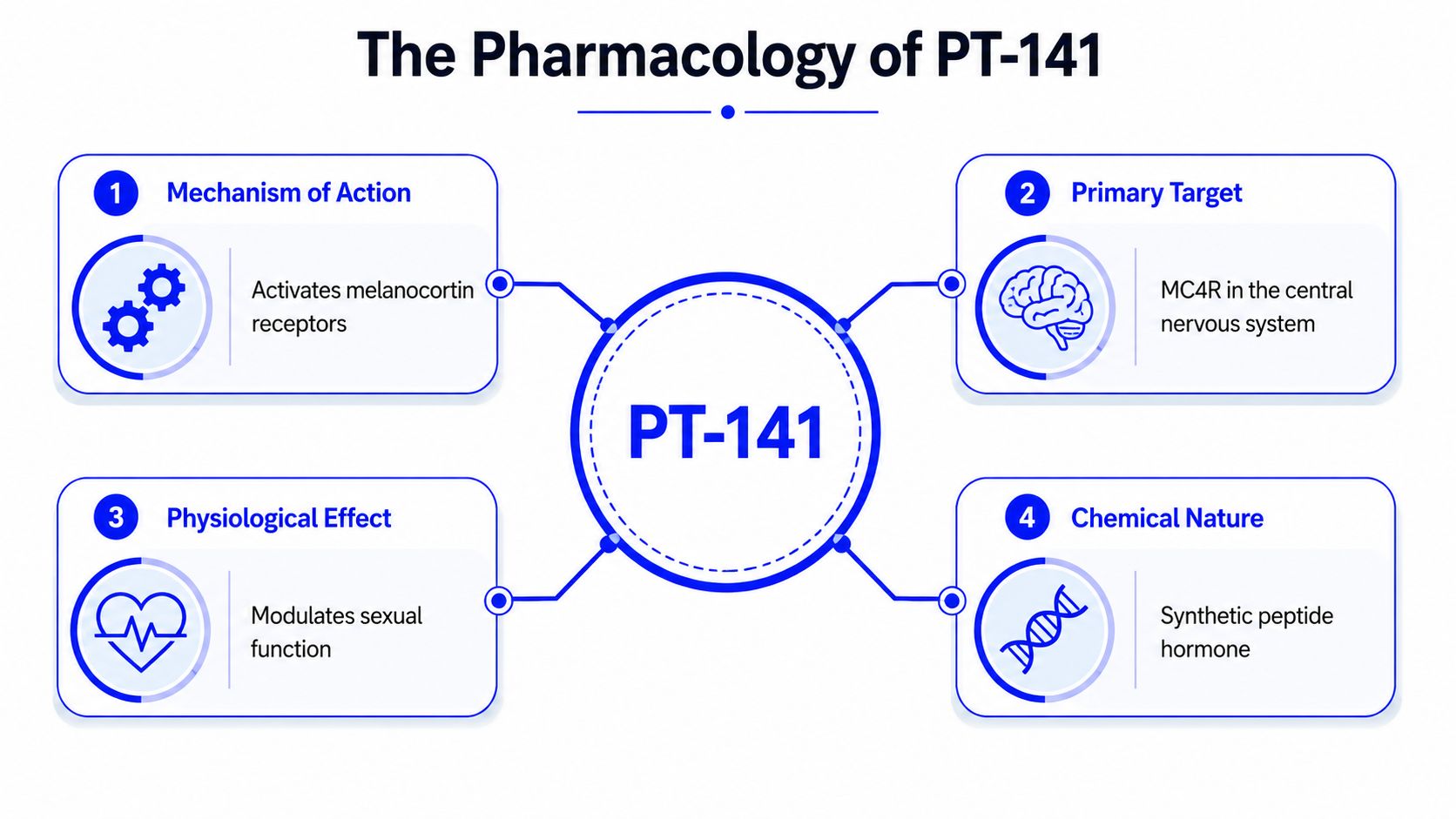
PT-141 nasal spray sits at the intersection of peptide pharmacology and formulation science. PT-141, also called bremelanotide, is a melanocortin receptor agonist studied for centrally mediated sexual-function pathways rather than the blood-flow pathways that dominate many older compounds. That distinction is useful in research. It also means formulation choices can change what you think you’re measuring.
If you’re evaluating PT-141 for laboratory, analytical, or preclinical work, the right question isn’t just “Does nasal delivery work?” It’s “What experimental trade-offs does nasal delivery introduce, and are those trade-offs acceptable for this protocol?” That’s where many new researchers get stuck.
A new lab member usually notices the same thing first. A nasal spray looks easier than a vial of lyophilized peptide that needs careful reconstitution and exact handling. That instinct isn’t wrong, but it’s incomplete.
With PT-141, the route of delivery can shape the quality of the data almost as much as the compound itself. A spray format may reduce handling steps, but it can also introduce uncertainty in droplet formation, mucosal deposition, and absorbed dose. If your endpoint is sensitive to timing or exposure, those variables matter.
PT-141 has legitimate scientific interest because it doesn’t primarily act like a classic peripheral vasodilator. Researchers study it as a synthetic melanocortin agonist with central nervous system activity. That makes it relevant when a project is exploring signaling pathways tied to arousal, motivation, or response patterns that aren’t explained by blood flow alone.
Practical rule: Don’t treat PT-141 nasal spray as “injectable PT-141 in a more convenient package.” Treat it as a different formulation problem with a different error profile.
That mindset changes protocol design. Instead of asking only whether the peptide is active, you start asking whether the dosage form is reproducible enough for your model, whether onset timing is tight enough for your observation window, and whether the material is standardized or compounded.
Three issues usually deserve the most attention:
Researchers who keep those distinctions clear usually build cleaner studies and spend less time troubleshooting noise that came from the dosage form rather than the peptide.
PT-141, or bremelanotide, is best understood first by what it is not. It is not primarily a blood-flow enhancer in the same sense as PDE-5 inhibitors. It is a melanocortin receptor agonist that acts mainly through the central nervous system, which is why it attracts interest in models where neural signaling is part of the hypothesis.
Think of two very different ways to influence a system. One approach changes the plumbing. The other changes the command signal. PT-141 belongs much closer to the second category.
That difference matters because it can produce useful research behavior even when a blood-flow-only strategy doesn’t explain the response. In a PubMed-indexed 2005 clinical study of intranasal PT-141 with sildenafil, the combination produced a significantly greater erectile response than sildenafil alone, and it was reported as safe and well tolerated without new or more frequent adverse events. For a researcher, the main takeaway isn’t promotional. It’s mechanistic. PT-141 appears to engage a pathway that can augment response when peripheral vascular modulation isn’t enough.
When you’re training on this compound, it helps to separate four layers of thinking:
| Research question | PT-141 framing |
|---|---|
| What class is it? | Melanocortin receptor agonist |
| Where does it mainly act? | Central nervous system |
| Why is that distinctive? | It isn’t limited to a peripheral blood-flow model |
| What does that change experimentally? | You may need to pay closer attention to timing, behavioral endpoints, and formulation-dependent exposure |
A beginner mistake is assuming that “sexual-function research compound” tells you enough. It doesn’t. Mechanism determines what controls you need.
For PT-141, useful controls may include route-specific comparisons, observation windows that capture central onset rather than only late physiologic effects, and careful interpretation when combining it with compounds that work through other pathways.
Treat PT-141 as a signaling probe first and a convenience product second. That framing usually leads to better experimental discipline.
PT-141 has moved far enough through the development pipeline that researchers aren’t working in a vacuum. There’s a real history here, and that history helps place laboratory questions in context.
PT-141, also known as bremelanotide acetate, reached an important regulatory milestone when it was approved by the FDA in June 2019 under the brand name Vyleesi for hypoactive sexual desire disorder in premenopausal women, as described in this clinical guide to PT-141 and bremelanotide. That approval matters for researchers because it confirmed serious clinical interest in a centrally acting melanocortin-receptor agonist rather than a purely vascular intervention.
That history also helps explain why PT-141 is often discussed across more than one study domain. It sits in a category where neurobehavioral signaling, sexual-function endpoints, route of administration, and tolerability all intersect. Few compounds bring those questions together in exactly the same way.
In research settings, PT-141 is commonly relevant to questions such as:
A lot of confusion comes from mixing three separate ideas. First, there’s the approved clinical identity of bremelanotide. Second, there’s the older intranasal research interest. Third, there’s the present-day reality that many researchers encounter PT-141 in nonstandardized formats. Those aren’t interchangeable categories.
Regulatory history tells you the compound is real. It doesn’t tell you that every current formulation on the market is equivalent for research purposes.
That distinction is where strong experimental design starts. If your work depends on reproducible exposure, the formulation itself becomes part of the scientific question, not just a procurement detail.
Most formulation discussions stop at convenience. That’s not enough for research work. The better question is which format introduces the fewest uncontrolled variables for your endpoint.
For many labs, the core comparison isn’t “spray versus injection.” It’s nasal spray versus lyophilized peptide prepared under controlled conditions. Those formats differ in handling, but a key difference is how much uncertainty they introduce.
A clinical overview of PT-141 for men and intranasal use notes a critical point for researchers. While intranasal PT-141 appeared in studies, no commercially standardized nasal spray exists for patients, and compounded sprays may have variable consistency and absorption. The same overview notes that injections are often preferred in clinical settings because intranasal delivery historically raised more concern about side effects and variable exposure.
That single point changes how a researcher should compare options.
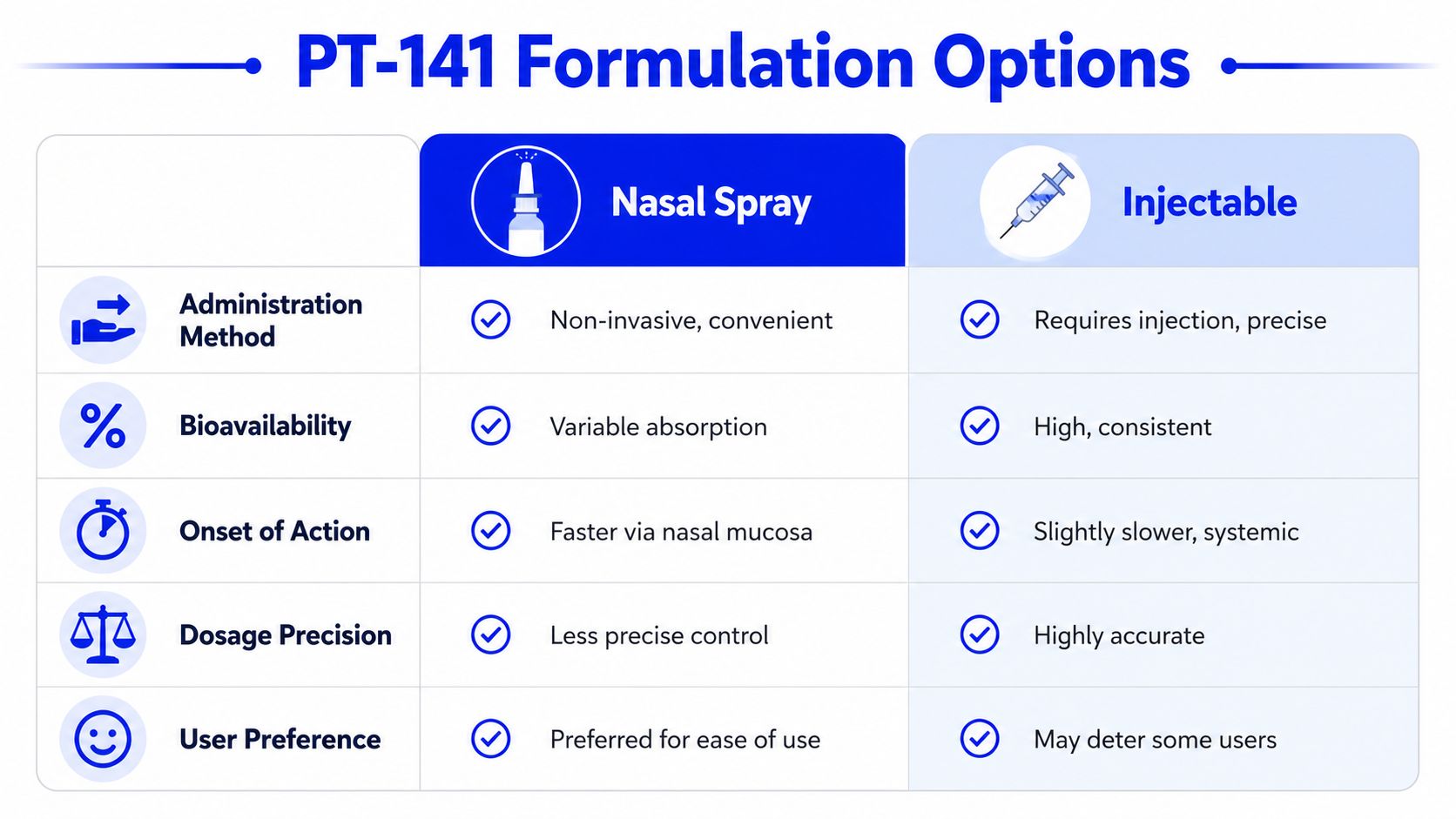
Here’s a practical comparison that reflects research priorities more than marketing language:
| Criterion | Nasal spray | Lyophilized or injectable-oriented preparation |
|---|---|---|
| Administration | Simple, noninvasive, fast to use | More handling, more training required |
| Dose precision | Depends on spray device performance and formulation uniformity | Usually easier to control analytically |
| Exposure predictability | Can vary with mucosal conditions and spray deposition | Often more consistent once prepared correctly |
| Stability concerns | Ready-to-use liquid introduces storage and degradation questions | Dry peptide often offers cleaner storage control before reconstitution |
| Best fit | Exploratory or convenience-driven workflows | Studies where reproducibility is the highest priority |
None of that means nasal spray is a poor research tool. It means you have to use it for the right reason.
Use a spray format when the route itself is part of the question, when noninvasive administration matters to the model, or when you’re specifically studying on-demand intranasal delivery. Prefer a lyophilized format when you need tighter analytical control over concentration, solution preparation, and dosing consistency.
Researchers also forget a simple but important point. A liquid peptide product is already a formulation decision. Someone has chosen the solvent system, concentration target, container type, and storage assumptions for you. If that information isn’t transparent, your experiment starts with hidden variables.
Dose planning for PT-141 nasal spray should begin with restraint, not ambition. The most useful published information points to a dose-response relationship, which means sloppy escalation can confuse interpretation instead of clarifying it.
A research-focused review of PT-141 nasal spray versus injection describes intranasal PT-141 effects beginning in 30 to 60 minutes for many users, with early higher-dose studies using 7.5 mg, 10 mg, 12.5 mg, and 15 mg and reporting better erectile outcomes than placebo. That same review notes one report in which erections lasted 5.3 times longer on average at higher intranasal doses. It also describes clinically relevant nasal spray use around 1.75 to 2 mg per dose, generally administered 30 to 60 minutes before activity and used only a few times per week.
For research interpretation, the important part isn’t the headline effect. It’s the pattern. PT-141 appears sensitive to dose and formulation context, which means you can’t assume that one intranasal concentration maps cleanly onto another.
A careful protocol usually follows a sequence like this:
Researchers should also account for the safety constraints associated with intranasal use. A prescribing-oriented PT-141 nasal spray reference describes on-demand use, administration roughly 30 to 60 minutes before sexual activity, dose ranges around 1.75 to 2 mg per dose, and use limited to a few times per week. It also flags concerns including increased blood pressure, nausea and vomiting, and avoidance in subjects with uncontrolled hypertension or significant cardiovascular disease.
Lab note: If your protocol records only the intended dose and not the observed tolerability signals, you may miss the reason a response curve looks irregular.
For non-clinical work, the right lesson is simple. PT-141 isn’t just dose dependent. It’s route dependent, formulation dependent, and observation-window dependent. Protocols need to reflect all three.
Liquid peptide formulations reward careful handling and punish casual storage. PT-141 nasal spray is no exception.

The practical goal is simple. Keep the peptide environment as stable as possible from receipt through use.
For any PT-141 nasal spray workflow, researchers should control:
Peptides in liquid form generally face more stability pressure than dry material. Heat, light, oxidation, and repeated handling can all reduce confidence in the sample over time. That doesn’t mean every stored spray degrades quickly. It means the burden of proof sits with the lab to document conditions carefully.
Storage practice should sit inside a documented chemical-safety framework, not a lab habit passed from one person to the next. If your team maintains internal safety files, the Annex II SDS compilation guidelines are a useful reference for understanding how safety data sheets should be structured and what information should be present.
A short visual review can help standardize handling habits across the bench team.
Watch for simple warning signs in stored solutions. Unexpected appearance changes, unclear labeling history, or uncertainty about storage interruptions should all trigger caution. In peptide work, “probably fine” isn’t a quality standard.
The fastest way to ruin a PT-141 study is to assume the label tells the whole story. It doesn’t. A peptide lot is only as trustworthy as the documentation behind it.
A Certificate of Analysis, or COA, is the minimum document a serious researcher should review before using a peptide lot. It should identify the material, connect it to a lot number, and show the analytical basis for the supplier’s claims.
For PT-141 or any comparable peptide, look for:
If any of those pieces are missing, your confidence in the material should drop immediately.

A good peptide package usually includes more than a COA. Researchers should also ask whether the supplier provides third-party support documents such as microbial and endotoxin reporting, especially when consistency and contamination control affect the study design.
Here’s the practical standard I’d hand to any new lab member:
A peptide isn’t “high quality” because a website says so. It’s high quality when the lot can be traced, the testing is legible, and the paperwork matches the material in your hand.
You should also think about traceability operationally, not just analytically. Can you connect the received bottle or vial to a purchase record, a lot record, a storage log, and a test document without guessing? If not, reproducibility gets weaker even before the experiment starts.
For PT-141 nasal spray, this matters even more because formulation variables already add uncertainty. If the dosage form may vary, the raw material and batch documentation need to be stronger, not weaker.
A reliable sourcing checklist usually includes these questions:
That’s not bureaucracy. That’s experimental control.
PT-141 nasal spray is scientifically interesting because its mechanism is central, not only vascular. That makes it useful for specific research questions, but it also makes formulation quality especially important. The nasal route may offer convenience, yet convenience can come with trade-offs in predictability, stability, and dose consistency.
Researchers usually get the cleanest outcomes when they treat PT-141 as both a pharmacology problem and a formulation problem. Keep route, storage, documentation, and traceability under tight control. And keep every decision inside a clear research-use-only framework.
If you’re looking for research-grade peptide options with lot documentation, transparent testing, and a catalog built for laboratory workflows, you can learn more at Peptide Warehouse USA and explore options that fit analytical and preclinical research needs.



