No products in the cart.
Most pages ranking for TB 500 peptide dosage start with a number. That’s the wrong starting point.
The more honest question is whether any human dose is evidence-based. Current summaries of the literature note that TB-500 is widely discussed as a synthetic analog related to thymosin beta-4, but there are no FDA-approved human dosing guidelines and the human data remain very limited, with most discussion built on preclinical work and informal practice patterns rather than validated standards, as noted by Paragon Sports Medicine’s TB-500 overview.
That matters because dosage isn’t just an amount. In research, dosage means a full protocol. You define the compound, model, route, frequency, exposure window, monitoring plan, and documentation standards before you ever write down a milligram figure.
A careful reader should treat online dose schedules as provisional. They may reflect what people repeat, not what controlled human evidence has established. If you’re trying to understand TB-500 intelligently, the useful skill isn’t memorizing a popular schedule. It’s learning how researchers think through dose selection when the literature is incomplete.
This guide takes that research-first approach. It explains what TB-500 is, how experimental dose logic is built, why route and timing matter, how labs think about translating animal work to a human-equivalent framework, and what safe handling and procurement should look like in a serious research setting.
People searching for a definitive TB 500 peptide dosage usually expect a clean answer such as one amount per week, one cycle length, and one maintenance phase. That expectation doesn’t match the state of the evidence.
TB-500 sits in an unusual category. It’s discussed constantly in wellness, fitness, and peptide circles, but it still lacks the one thing many readers assume must already exist: a validated, broadly accepted human dosing standard. That gap changes how an educator should answer the dosage question.
Most online dosage articles compress a complicated research problem into a consumer-style recommendation. They skip the hard parts: what biological endpoint is being studied, how exposure is maintained, what route is used, whether the protocol is derived from animal work, and what level of uncertainty remains.
A serious protocol starts by asking:
Practical rule: If a dose recommendation appears without context on route, frequency, rationale, and monitoring, it isn’t a protocol. It’s a number detached from method.
The right way to think about TB-500 dosage is methodological rather than formulaic. You build from mechanism, then preclinical evidence, then translational reasoning, then administration design, then quality control.
That approach won’t give everyone the same number, and that’s the point. In peptide research, uncertainty has to stay visible. When the literature is thin, pretending certainty exists is the fastest way to design a poor protocol.
TB-500 is generally discussed as a synthetic analog or fragment related to thymosin beta-4, a naturally occurring peptide associated in the literature with repair-related biology. That connection is why TB-500 is repeatedly explored in discussions of tissue recovery, cell movement, and healing-related signaling.
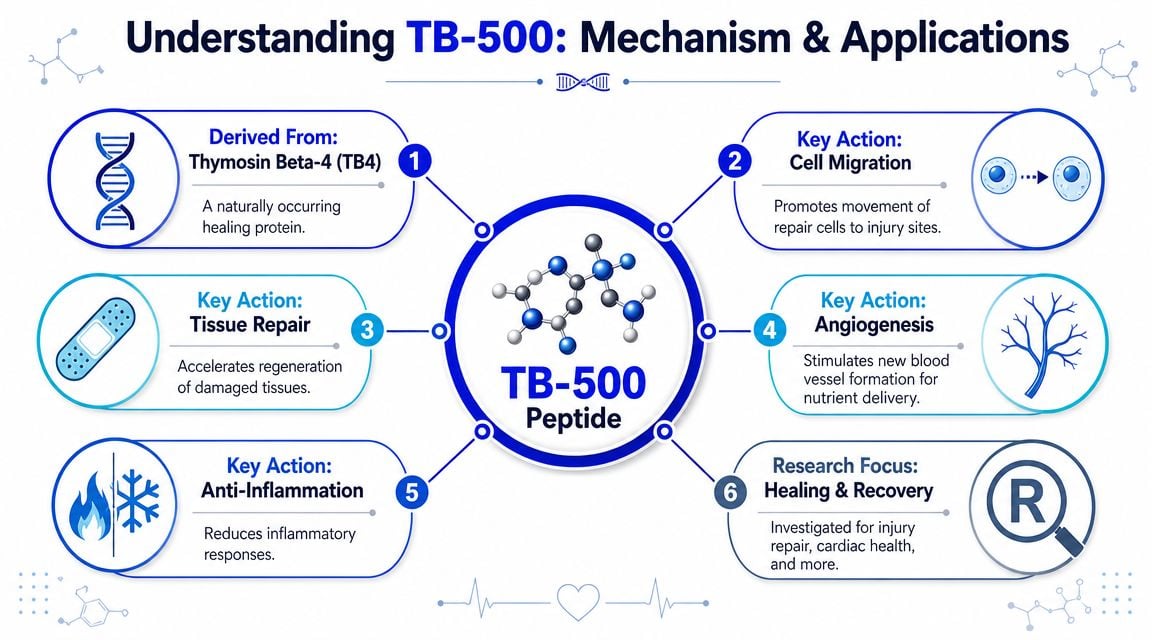
The simplest way to explain TB-500 to a new lab member is this: researchers are interested in it because it’s associated with biological processes that support cell migration and repair signaling. Those processes matter in studies involving damaged tissue, recovery models, and regenerative hypotheses.
You’ll often see four ideas appear together in TB-500 discussions:
For readers who want a broader clinical context around recovery science, it can also help to explore regenerative medicine advances in a setting where repair-focused therapies are discussed more broadly.
Mechanism doesn’t tell you the exact dose, but it tells you what kind of dosing logic might make sense. If a compound is being studied for signaling related to migration and repair, then the protocol may focus less on a single large administration and more on how consistently the tissue sees the compound over time.
That’s a different mindset from typical drug-label thinking. With TB-500, people often search for one “correct” amount. In a research framework, the better question is whether the administration pattern matches the biological process being studied.
A short primer can help visualize that distinction:
A mechanism hypothesis is not proof of a finished human protocol. It only gives you a reason to investigate. That’s why good researchers separate three things that often get blurred together online:
| Term | What it means in practice |
|---|---|
| Mechanism | A biologic rationale for why the peptide might matter |
| Protocol | A structured plan for route, timing, exposure, and observation |
| Recommendation | A validated standard suitable for routine human use |
TB-500 has plenty of discussion in the first category, some activity in the second, and much less certainty in the third.
If you want to understand why TB-500 dosage claims vary so much, start with the source material. Most dosage discussion doesn’t come from a substantial body of standardized human trials. It comes from a mix of preclinical reasoning, extrapolation, and repeated informal schedules.

The figures repeated most often in major English-language wellness and sports-medicine content tend to cluster around 2 to 5 mg per injection or 4 to 8 mg total per week, commonly via subcutaneous or intramuscular administration, with many protocols lasting 4 to 12 weeks. One guide described an initial phase of 2.0 to 2.5 mg every other day, a weekly total of 4 to 8 mg split across 2 to 3 administrations, and a later reduction to 2 to 6 mg per month after improvement. Another overview cited 5 mg to 20 mg per week as typical. The key caution is that these are described as a market consensus built from anecdotal practice patterns rather than approved-label dosing from rigorous human trials, as summarized by HubMedEd’s TB-500 dosing overview.
That single point explains a lot. Many readers assume repeated numbers must equal established science. Sometimes repeated numbers just mean repeated copying.
In preclinical work, dosage is usually tied to the design of a specific model. Researchers choose an exposure strategy to test a question. They are not necessarily trying to create a general human-use recommendation.
When reviewing preclinical literature, pay attention to these filters:
Animal data are useful for generating hypotheses. They are weak tools for pretending a consumer-ready human dosage already exists.
Treat commonly cited schedules as signals of what the market repeats, not proof of what’s settled. That distinction protects you from a common mistake: confusing popularity with validation.
A more defensible reading looks like this:
| Evidence type | What it can support | What it cannot support |
|---|---|---|
| Anecdotal protocol pattern | Identifying common practice language | Establishing a validated human standard |
| Preclinical model result | Building a translational hypothesis | Proving a final human dose |
| Repeated online schedule | Showing what people tend to copy | Confirming that the schedule is optimal |
That’s the frame a careful researcher keeps in mind before moving into any dose translation exercise.
A common beginner mistake is simple weight matching. If an animal model used a certain amount per kilogram, a novice may try to multiply that number directly by human body weight. That shortcut ignores differences in metabolism, surface area, and species-specific pharmacology.
Allometric scaling exists because organisms of different sizes don’t process compounds in a linear, body-weight-only fashion. A dose that works as an experimental exposure in a small animal doesn’t translate cleanly by arithmetic alone.
In practical terms, scaling is a framework for estimating a human equivalent dose, often abbreviated HED. It is not a prescription and it is not a validated recommendation. It’s a research tool for planning and interpretation.
Use allometric thinking for:
Because the verified data here do not provide a specific animal-study mg/kg figure or conversion factor, the responsible approach is to show the structure of the calculation without inventing numbers.
The logic usually follows this sequence:
Here is the framework in table form.
| Parameter | Value | Calculation/Note |
|---|---|---|
| Animal species | Rat | Use the exact species reported in the study |
| Animal dose | Study-specific | Record the published mg/kg dose exactly |
| Scaling approach | Allometric scaling | Do not use direct body-weight matching alone |
| Human equivalent dose | Derived estimate | Convert animal mg/kg to human-equivalent mg/kg using the selected scaling method |
| Target body weight | Study-specific | Apply only after human-equivalent mg/kg is estimated |
| Final nominal amount | Calculated output | Treat as a theoretical research starting point, not an approved human dose |
| Route adjustment | Required | Reassess if route differs between the animal model and proposed protocol |
| Frequency adjustment | Required | Exposure pattern may matter as much as nominal amount |
Lab note: A well-documented estimate is still only an estimate. Scaling reduces one type of error. It doesn’t remove biological uncertainty.
The numeric conversion is only the midpoint of the job. You still need to ask whether the animal study used the same route, whether the peptide exposure was acute or repeated, whether tissue targeting differs, and whether the outcome measure in that model is even relevant to your intended question.
That’s why two competent researchers can look at the same preclinical paper and design different provisional protocols. The calculation matters, but interpretation matters just as much.
Amount alone never tells the full story for TB 500 peptide dosage. Route and timing shape the exposure profile, and exposure profile shapes what the experiment is really testing.
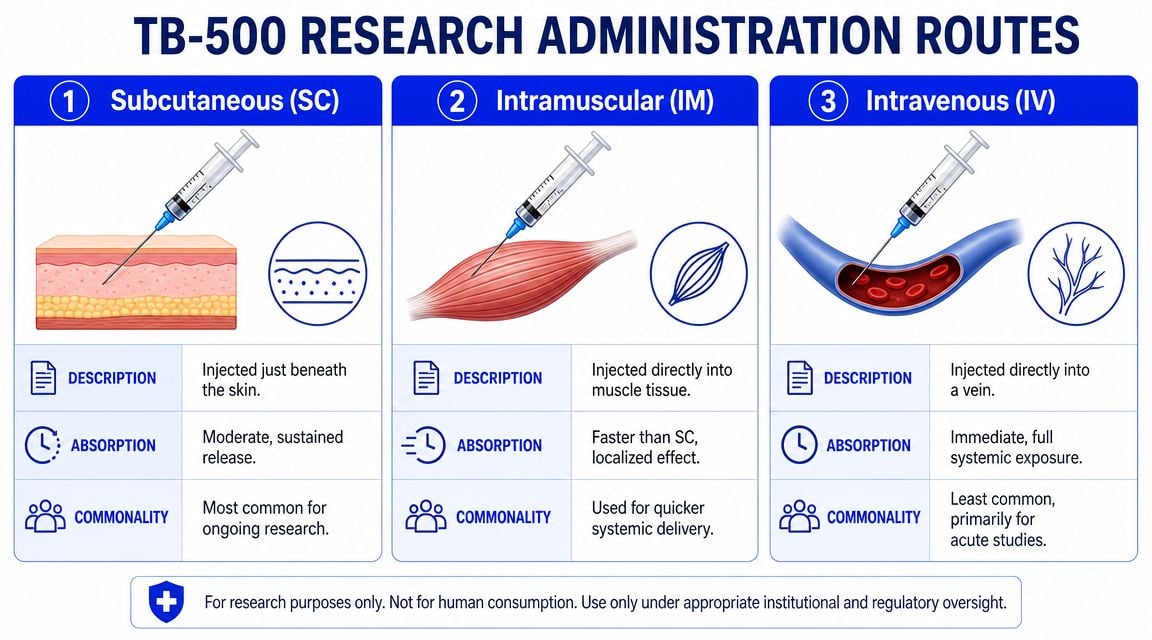
In practice, research discussions usually focus on three administration routes. Each has a different logic.
| Route | General use logic | Practical trade-off |
|---|---|---|
| Subcutaneous SC | Common when researchers want manageable, repeatable administration | Slower uptake than direct vascular delivery |
| Intramuscular IM | Sometimes chosen when local tissue context is part of the design | Technique consistency matters |
| Intravenous IV | Used when immediate systemic exposure is the main objective | More demanding handling and less common in routine peptide discussions |
Route changes interpretation. If one protocol uses SC and another uses IM, matching the milligram figure alone can mislead you because the tissue exposure pattern may not be equivalent.
Independent peptide-therapy summaries commonly describe use around 2 to 5 mg per week, often split into one to three injections, with some protocols extending across 6 to 12 weeks and then stepping down to maintenance. Other overview sources describe once-daily subcutaneous use five days per week rather than one weekly bolus. The rationale often given is pharmacologic rather than cosmetic: TB-500 is described as having a short half-life of about 2.5 to 3 hours after subcutaneous administration, so dividing administration across the week is intended to reduce peak-trough swings and maintain more stable signaling related to migration and repair. These same summaries also note local irritation and symptoms such as fatigue, headache, or nausea as the main tolerability issues reported in non-controlled use, as described by Innerbody’s overview of thymosin beta-4 and TB-500.
That half-life point is easy to misunderstand. It doesn’t mean “inject more.” It means protocol designers often think about stability of exposure instead of just the size of a single administration.
Online protocols often mention “loading” and “maintenance” phases. Those terms can be useful shorthand, but they can also hide sloppy thinking.
A proper use of those labels would mean:
Without those details, phase language sounds scientific without being rigorous.
A protocol can fail before the first administration if the material is poorly sourced or badly handled. With peptides, quality control is part of dosage control. If identity, purity, or storage conditions are uncertain, your nominal dose may not reflect the actual material in the vial.
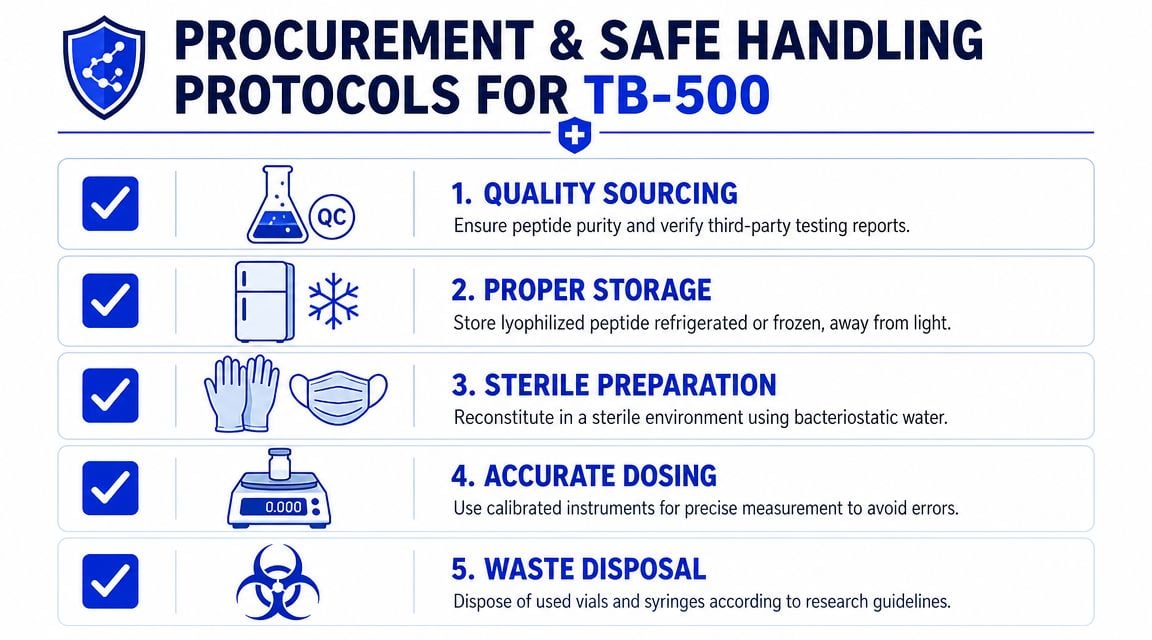
Treat procurement like incoming materials review, not shopping.
Use a checklist:
The cleanest-looking vial tells you almost nothing by itself. Documentation is what makes a research material auditable.
Peptides are easy to degrade through casual handling. Teams lose protocol reliability when they treat storage and preparation as housekeeping instead of experimental control.
A disciplined handling routine usually includes:
Many “dose problems” are handling problems. A protocol may look inconsistent because the peptide wasn’t stored properly, the reconstitution record is incomplete, the measuring tool wasn’t calibrated, or a vial from a different lot was substituted without documentation.
That’s why procurement and handling belong in any dosage conversation. Dose isn’t only what you planned to administer. Dose is what the material was, how it was prepared, and whether your records prove it.
TB-500 should be discussed with regulatory precision. It is not an FDA-approved medicine, and that fact shapes every responsible conversation about dosage.
There is no established, evidence-based human dosage for TB-500 because it is not an FDA-approved medicine. A 2021 review noted that TB4 or TB-500 was “well tolerated and safe in healthy people” in limited studies, but that observation is not the same as a validated dosage recommendation for consumers or patients, as summarized in this evidence overview on TB-500 and BPC-157 dosing in humans.
That distinction is critical. Tolerability in limited research does not create an approved schedule, a standard cycle, or a consumer-use instruction set.
A compliant, ethical way to talk about TB-500 should always keep these boundaries visible:
If someone presents TB-500 as if it already has a settled, label-like human dosage, they’re overstating the evidence.
The useful answer to TB 500 peptide dosage isn’t a single number. It’s a method.
A careful approach starts with mechanism, checks what preclinical evidence supports, translates animal data cautiously rather than casually, and then builds a route-and-frequency plan that matches the exposure goal. After that, quality control and documentation determine whether the protocol is even interpretable.
That’s the difference between research and repetition. One produces defensible records. The other produces internet folklore.
If you’re evaluating peptides for laboratory, analytical, or preclinical work, high-quality sourcing and transparent batch documentation should sit at the center of your process, not at the end.
Researchers who need documented peptide sourcing can learn more at Peptide Warehouse USA, where the focus is on USA-made research materials, transparent batch records, COAs, and laboratory-use procurement standards. Explore options if your work depends on traceability, consistency, and research-use-only compliance.



