No products in the cart.

You’re probably seeing the term Tesa IPA blend in supplier catalogs, forum threads, and product pages that promise broad benefits of peptides, yet give very little detail about what the material is in a lab setting. That gap matters. If you’re evaluating a vial for receptor work, pathway analysis, or metabolic research, marketing language is noise. What you need is a clear account of composition, mechanism, handling, and the limits of what current evidence can support.
In research use, the Tesa IPA blend refers to a combined preparation of Tesamorelin and Ipamorelin. The blend is mainly discussed in relation to growth hormone signaling, metabolic pathway modeling, and the study of pulsatile secretory responses. The useful question isn’t whether the blend sounds promising. The useful question is whether the material, protocol, and interpretation are scientifically tight enough to justify the experiment.
In a research context, the Tesa IPA blend is a paired peptide system built from Tesamorelin and Ipamorelin. Researchers usually encounter it when studying coordinated stimulation of growth hormone pathways rather than a single receptor target. That distinction matters because the blend is discussed very differently in marketing copy than in technical work.
The operational baseline is simple. This material belongs in preclinical research and in vitro studies, not in consumer wellness language. Supplier labeling explicitly states that the Tesa-Ipa blend is designated exclusively for preclinical research and in vitro studies, and that it is not approved for human consumption, veterinary use, or therapeutic application, with use requiring compliance with institutional research guidelines, as described on the Tesamore and Ipamorelin product listing.
Practical rule: If a protocol can’t be defended as laboratory, analytical, or preclinical work, the material is being discussed in the wrong context.
That research-only framing helps clear up two common points of confusion:
A lot of content treats the blend as if mechanism, purity, protocol, and interpretation are all settled. They aren’t. Some supplier documentation describes lyophilized research material with ≥99% purity, combining 5 mg Tesamorelin and 5 mg Ipamorelin per vial, and emphasizes lawful laboratory use only, as noted in the Tesamorelin Ipamorelin blend technical description.
That’s a useful starting point for lab personnel because it shifts the conversation from hype to fundamentals:
A vial labeled “tesa ipa blend” can look straightforward until you ask a basic lab question: which signal is doing what? If that question stays blurry, the rest of the experiment usually does too. The blend combines two peptides that sit in the same hormonal network but act at different control points, so clear interpretation starts with separating their roles before considering them together.
Tesamorelin is a GHRH analog. In research terms, that means it is used to engage the growth hormone releasing hormone receptor and provide an upstream stimulus to pituitary somatotroph function.
For experimental design, Tesamorelin matters because it gives you a defined entry point into the axis. It behaves less like a general pressure on secretion and more like a receptor-directed instruction. If a readout shifts after Tesamorelin exposure, the first interpretation to test is altered GHRH receptor signaling, not an undefined global effect.
That distinction helps with controls. A technician comparing Tesamorelin alone versus the blend is not comparing “weak” and “strong.” The comparison is between a single upstream cue and a multi-input system.
Ipamorelin is commonly described as a ghrelin-pathway agonist or mimetic, with activity associated with GHSR-related signaling. Its role in a blend is different from Tesamorelin’s role. It does not replicate the GHRH signal. It adds a second regulatory input that can change the pattern, magnitude, or timing of secretory responses.
A practical analogy helps here. Tesamorelin sets one control dial. Ipamorelin adjusts a second dial on the same instrument panel. If both dials move at once, the output may rise, but the more important laboratory question is whether the pulse pattern also changes.
That is why selectivity claims need careful handling. Receptor selectivity narrows one part of the mechanism. It does not guarantee simple downstream behavior in a co-formulated system. Once two peptides converge on related endocrine circuitry, attribution becomes harder, not easier.
Researchers who need a refresher on the signaling background often benefit from seeing ghrelin and leptin explained in broader endocrine context, especially to avoid treating ghrelin-associated signaling as interchangeable with every other metabolic input.
| Characteristic | Tesamorelin | Ipamorelin |
|---|---|---|
| Core role | GHRH analog | Ghrelin-pathway mimetic |
| Primary pathway emphasis | GHRH receptor activation | GHSR-related signaling |
| Research value | Defines an upstream pituitary stimulus | Modifies secretory responsiveness |
| Common reason for inclusion in a blend | Establishes the initiating cue | Adds a second regulatory input |
| Interpretation challenge | Separating receptor-driven effects from downstream cascade effects | Distinguishing amplification from an independent contribution |
The blend gets attention because it is a dual-pathway research model. This is the scientific interest, not the product language that often surrounds it. Combining Tesamorelin and Ipamorelin allows investigators to examine how GHRH-receptor signaling behaves when a ghrelin-receptor-related input is present at the same time.
This matters for study design. If the output changes under co-exposure, the result may reflect altered pulse architecture, shifted receptor cooperation, or timing effects within the secretory cascade. A stronger endpoint alone does not tell you which of those happened.
For that reason, the blend is best treated as a system for mechanism studies rather than a shortcut to broad conclusions. Useful experiments usually depend on matched single-agent controls, sampling windows that can resolve pulsatile effects, and endpoint selection that separates signal initiation from signal amplification.
The cleanest way to think about the Tesa IPA blend is as a two-receptor system. One peptide turns on a known upstream signal. The other reinforces the secretory response through a separate route. Researchers who miss that architecture often design experiments that blur cause and amplification.
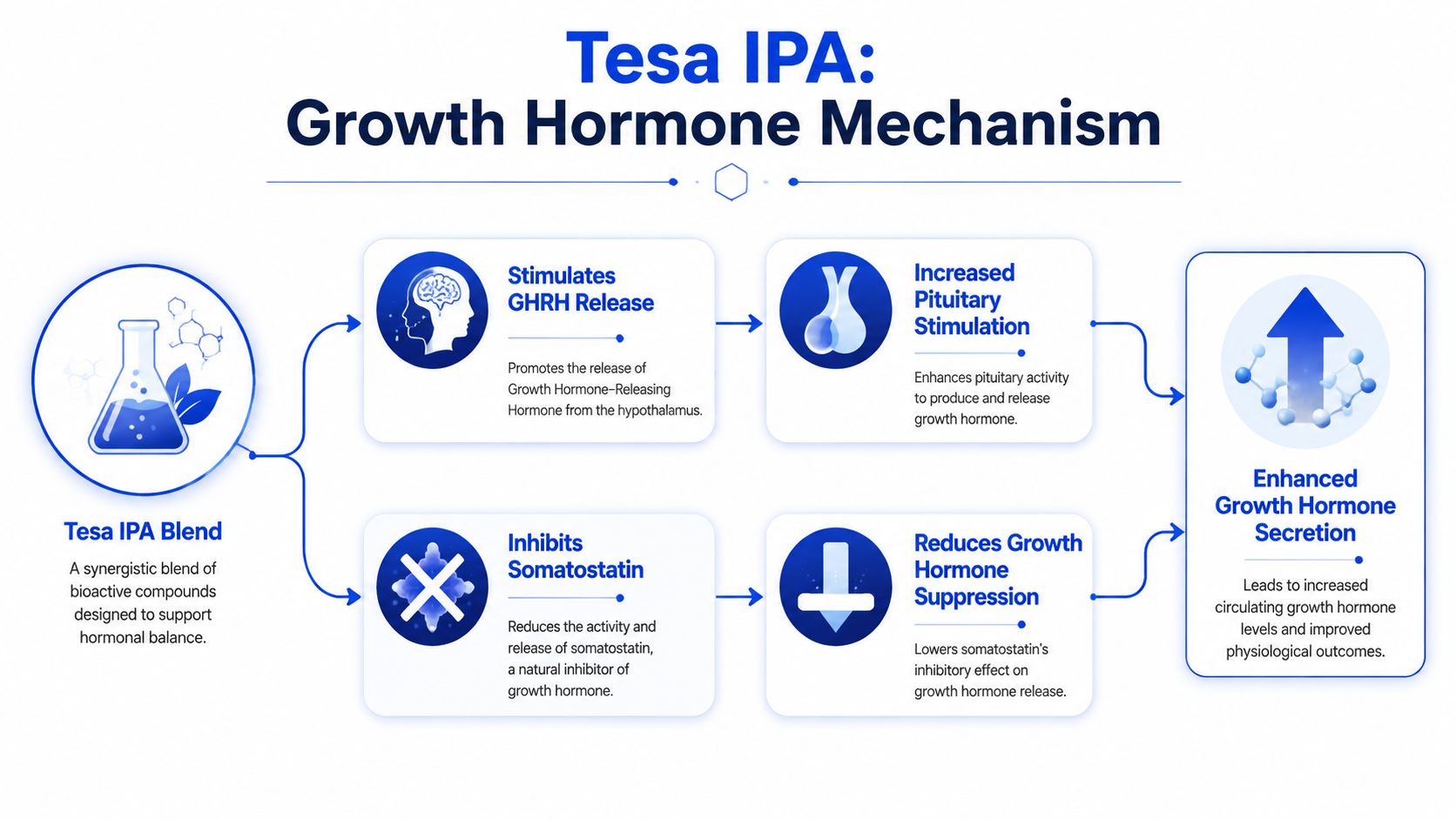
Tesamorelin acts on the GHRH receptor in pituitary somatotrophs. That signal favors growth hormone synthesis and release. If you want a simple analogy, Tesamorelin is the first key. It engages the primary lock.
Ipamorelin engages the ghrelin receptor pathway, often discussed as GHSR signaling. That creates a second input that can amplify GH release and alter pulse behavior. In the two-key analogy, Ipamorelin doesn’t replace the first key. It opens a second lock that helps the system respond more strongly.
Receptor cooperation changes how you interpret a positive result. You aren’t seeing a single receptor pushed harder. You’re observing how two coordinated inputs modify the secretory pattern.
The value of the blend isn’t limited to GH output alone. It’s also a way to study signaling hierarchy, receptor interplay, and metabolic pathway response under controlled conditions. In practical terms, the blend gives a lab a model for asking whether a dual-input design changes timing, amplitude, or downstream markers compared with one-input designs.
A useful background resource for understanding why ghrelin-related signaling attracts so much interest is ghrelin and leptin explained. It helps frame why ghrelin-linked pathways are discussed so often in metabolism research, even though a research-grade peptide experiment still needs much tighter controls than consumer education content provides.
Mechanistic caution: When two peptides converge on one endocrine output, a larger response doesn’t automatically tell you which pathway drove the change. You need controls for each component and the combination.
A solid mechanism-focused workflow usually includes:
The Tesa IPA blend is usually discussed in studies tied to body composition, visceral adipose tissue, and metabolic signaling. Those are not interchangeable endpoints. A careful protocol defines which one matters before the first vial is reconstituted.

Clinical and preclinical protocol summaries commonly describe study durations ranging from 12 to 16 weeks, with noticeable reductions in visceral fat reported within an 8 to 12-week window in test subjects, according to the Beverly Hills Rejuvenation Center protocol overview. Those timelines are useful for experimental planning because they tell you the blend is typically evaluated over weeks, not in a short acute snapshot.
In a laboratory setting, the blend is often relevant when the research question sits at the intersection of endocrine signaling and metabolic outcome. Typical use cases include:
These are studied applications, not guarantees. In a well-run lab, each one becomes a separate hypothesis with separate endpoints.
Most useful studies don’t stop at a broad “did it work” question. They define measurable categories and stick to them.
A video overview can be helpful for orienting newer staff before they move into method-specific SOPs:
Don’t let broad outcome language flatten your study design. “Body recomposition” sounds efficient in marketing, but in a lab it’s several distinct measurement domains.
Many otherwise careful projects often get sloppy. A high-purity lyophilized peptide doesn’t produce reliable data on its own. Technique, calculation, labeling, and storage discipline do that.

Technical descriptions for research-grade material describe the blend as a lyophilized research compound intended for laboratory use, with documented batch production and traceability. Some product documentation specifies a vial composition of 5 mg Tesamorelin and 5 mg Ipamorelin, and emphasizes research-only restrictions, as noted earlier in the technical product description.
That sounds straightforward until the team starts converting vial content into working concentrations. Then the actual problems show up.
A frequently asked question concerns the precise, pharmacokinetically validated dosing protocols for converting milligram lyophilized powder into microgram injection volumes using bacterial water, and standardized, peer-reviewed guidance for this specific blend is lacking. That means each lab has to operate from validated internal calculations, COA review, and a documented SOP rather than generic internet charts.
A practical workflow looks like this:
“If the math lives only in someone’s head, the experiment isn’t reproducible.”
The most common mistake isn’t arithmetic. It’s treating all blended vials as if they behave like a single-compound standard. With a dual-peptide vial, you have to think about at least three variables:
| Error point | Why it matters | Better practice |
|---|---|---|
| Assuming universal reconstitution charts apply | Blend-specific guidance is limited | Build calculations from the actual vial content and internal SOP |
| Ignoring purity adjustments | Nominal mass and active mass may differ | Review lot-specific documentation before preparing working concentrations |
| Overlooking co-solution stability questions | Co-reconstituted peptides may not behave uniformly | Use a conservative handling window and document appearance and timing |
There’s another important limitation. Current discussion around this blend often skips the unresolved issue of variable stability and aggregation behavior when Tesamorelin and Ipamorelin are co-reconstituted in the same solution. That doesn’t invalidate the blend as a research tool. It does mean your handling protocol should be written with caution, not assumption.
A common lab scenario makes the problem clear. A vial arrives with polished language about synergy, optimization, and broad performance claims, yet the underlying support for the combined formulation is much thinner than the wording suggests. For a researcher, that mismatch is the first warning sign.
The central issue is not whether Tesamorelin and Ipamorelin have plausible biological activity. Each has a defined mechanistic rationale. The problem is that promotional claims about the blend often extend far beyond what has been documented for the combination over longer study periods, especially outside clearly defined disease contexts.
One question remains insufficiently resolved: What are the documented risks and limitations of repeated combined GHRH analog and ghrelin mimetic exposure in populations without the metabolic condition tied to Tesamorelin’s established clinical history? Current discussions often acknowledge that the combination has not been validated by major clinical trials for broad use in healthy populations, and they leave long-duration safety questions only partially addressed.
That uncertainty should change how claims are read. A plausible receptor-level model can justify a hypothesis. It does not validate a long-term research conclusion, and it certainly does not justify broad claims detached from population, endpoint, and study duration.
A plausible mechanism and a validated application are different forms of evidence.
Researchers see this distinction every day in other systems. Binding is not the same as downstream functional effect. Acute signaling is not the same as chronic adaptation. A dual-secretagogue concept may be mechanistically interesting, but without controlled evidence for the exact combined protocol under discussion, the responsible position remains narrow.
A disciplined review of any Tesa IPA blend product or protocol should ask:
Those questions matter because the two components do not enter the literature with equal evidentiary weight. Tesamorelin has a specific documented history in a defined clinical setting. Ipamorelin is primarily discussed as a research peptide. The blend is another category altogether. Combining two known agents does not automatically produce a well-characterized research tool. In peptide work, mixtures can introduce new interpretive problems, including altered handling assumptions, uneven evidence standards, and overconfident conclusions.
Language is often the easiest place to detect hype. Terms such as “clinically proven,” “synergistic optimization,” or “complete body recomposition support” compress multiple unanswered questions into a single polished phrase. A technically sound writeup should identify the exact population studied, the protocol used, the endpoint measured, and whether the evidence applies to one component or to the co-formulated blend itself.
The practical standard is simple. Treat the Tesa IPA blend as a research compound with an interesting dual-pathway hypothesis, not as a settled platform with established long-term outcomes. Build work around verified material identity, documented batch quality, narrow experimental endpoints, and conservative interpretation.
If the evidence chain is incomplete, the conclusion must stay narrow.
If you’re sourcing research peptides and want batch documentation, traceability, and a catalog built for laboratory use, learn more at Peptide Warehouse USA and explore options for research-grade materials backed by COAs and transparent lot support.



