No products in the cart.
You're probably looking at a vial label, a calculator, and three conflicting protocol pages, all trying to answer one practical question: what counts as a rational tesamorelin ipamorelin blend dosage for research? That confusion is common because the blend sits in an awkward middle ground. Tesamorelin has a documented clinical dosing history, while tesamorelin plus ipamorelin protocols are mostly framed as research practices rather than standardized therapy.
That gap matters. If you treat a blend protocol as though it carries the same evidentiary weight as tesamorelin alone, your study design can drift from pharmacologic logic into guesswork. If you ignore the reason people combine them in the first place, you miss the central hypothesis behind the stack.
A useful way to approach this topic is to separate three questions. First, what does each peptide do on its own? Second, why blend them at all? Third, how do publicly described research dosages compare with the much more established tesamorelin monotherapy baseline?
Most online discussions about peptide blends jump straight to injection volumes. That's the wrong starting point. A lab technician needs to know whether the protocol reflects an approved therapeutic standard, a commonly repeated research convention, or a theoretical stack built from mechanism-first reasoning.
That distinction is especially important with tesamorelin ipamorelin blend dosage. Tesamorelin has a documented regulatory history and a defined human dosing benchmark. The blend doesn't. So the dosage conversation isn't just about how much powder sits in the vial. It's about what level of evidence supports the amount, frequency, and purpose of the protocol.
Practical rule: Start with the peptide that has the strongest dosing anchor, then judge the blend against that anchor rather than the other way around.
In practice, that means treating tesamorelin as the reference compound. It gives you a real-world baseline for daily administration, a known indication, and a clearer framework for monitoring. Blend protocols then become a separate category: research-oriented, lower-dose, and more interpretive.
A disciplined workflow usually includes these checkpoints:
The most useful insight isn't that blends exist. It's that the blend should be treated as a hypothesis under investigation, not as an upgraded version of tesamorelin by default.
Tesamorelin and ipamorelin often get grouped together under the broad label of “GH peptides,” but that shorthand obscures the actual logic of the blend. They don't do the same job. They act on related signaling territory through different inputs, and that difference is the whole reason anyone combines them.
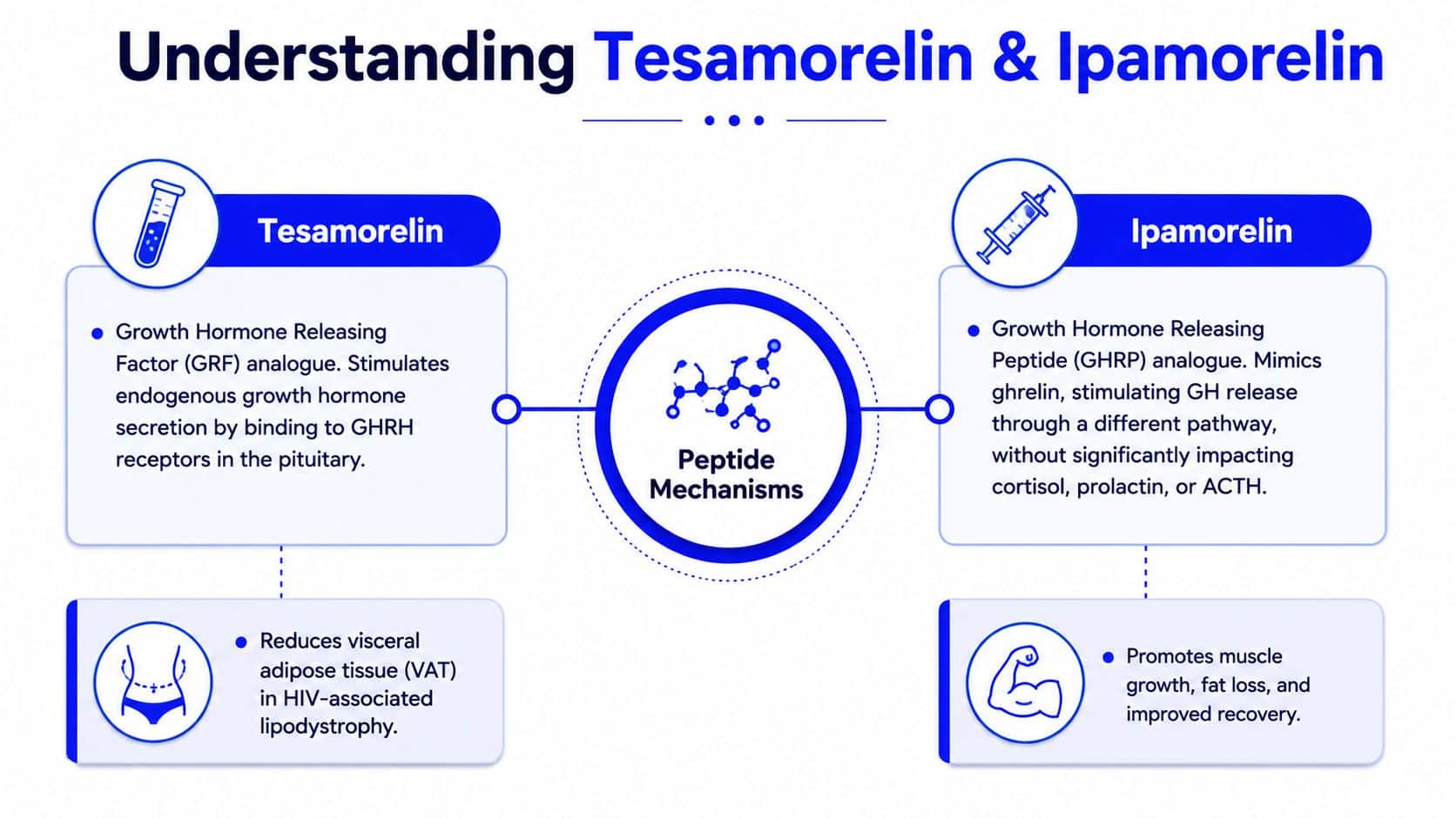
Tesamorelin is best understood as the peptide in this pair with the strongest clinical footing. The FDA prescribing information for EGRIFTA SV states that the product contains 2 mg tesamorelin per single-dose vial and that the recommended adult dose is 2 mg subcutaneously once daily for HIV-associated lipodystrophy. That labeling history traces back to 2010 in the United States.
Mechanistically, tesamorelin functions as a growth hormone-releasing hormone analog. In plain language, it acts like a signal requesting endogenous growth hormone release through the GHRH pathway. For a technician, the practical point is simple: tesamorelin is not being discussed in a vacuum. It already has a dosing and monitoring context.
That context shapes interpretation in two ways:
Ipamorelin is usually framed as a growth hormone secretagogue and a ghrelin-mimetic style signal. A useful lab analogy is that tesamorelin “requests” GH release, while ipamorelin “opens the gate” through a different stimulus channel. The two aren't duplicates. They are overlapping but non-identical prompts.
That difference is why researchers see the blend as attractive. If one peptide biases signaling through a GHRH-like route and the other stimulates release through a GHS-style route, combining them may create a more pronounced pulse than either input alone. That's the theory. It's also where many discussions stop too early.
The existence of two pathways doesn't automatically prove that combining both produces a better study outcome for every objective.
For technicians and protocol designers, the cleanest approach is to treat tesamorelin as the evidence-backed anchor and ipamorelin as the experimental amplifier. That framing keeps the mechanism clear and prevents the blend from being mistaken for an established standard.
The most common justification for combining these peptides is pathway complementarity. Tesamorelin is used to stimulate endogenous GH signaling through one upstream route. Ipamorelin is added to stimulate release through another. In theory, the blend is designed to make GH pulsing feel more physiologic and stronger than a single-input protocol.
This is the best version of the synergy argument. A GHRH analog and a secretagogue aren't identical tools, so a researcher may choose both when the study question centers on pulsatility, stacked signaling, or whether dual-pathway stimulation changes downstream observations.
That idea is plausible enough to explain the blend's popularity. It also explains why so much public content around the stack focuses on body-composition research, recovery discussions, and sleep-timed administration. The blend is not usually presented as a replacement for tesamorelin's approved indication. It is usually framed as an attempt to broaden or intensify the signaling pattern.
A technician should still ask a stricter question: what problem is the second peptide solving?
That question is where the discussion becomes more useful. The Mayo Clinic tesamorelin drug information reinforces that the strongest evidence base sits with tesamorelin as a single agent at 2 mg once daily. It also highlights commercially recognized daily dosing presentations and underscores that tesamorelin already carries a monitoring burden involving glucose, edema, and IGF-1-related concerns.
That leads to an under-discussed conclusion. For some research goals, adding ipamorelin may be mechanistically interesting but not necessarily necessary. If tesamorelin already targets the endpoint under investigation, the blend can make interpretation harder because you've introduced a second variable without standardized combination evidence.
Consider the tradeoff:
| Research question | Tesamorelin alone | Tesamorelin plus ipamorelin |
|---|---|---|
| Is the endpoint already aligned with tesamorelin's established profile? | Cleaner attribution | Harder attribution |
| Is dual-pathway GH signaling the actual object of study? | May be too narrow | Better fit for the hypothesis |
| Does monitoring complexity matter? | Lower complexity | Higher complexity |
Key distinction: Blending can be rational. It isn't automatically superior.
That's the nuance basic dosing guides miss. The primary decision isn't just “how much of the blend should be used?” It's “does the research question justify moving away from the peptide with the stronger standalone evidence base?”
Once you separate established tesamorelin use from experimental blend use, the dosage picture becomes easier to interpret. Publicly described blend protocols aren't built around matching tesamorelin's labeled monotherapy dose. They usually sit far below it.
The publicly described blend protocol summary reports that tesamorelin-ipamorelin blends often start around 300 mcg, escalate toward 500 mcg or 1 mg daily, and are commonly framed around 8–12 weeks or 5 days on, 2 days off schedules. It also notes that these protocols are generally much lower than the 2 mg/day FDA-labeled tesamorelin monotherapy amount, representing roughly 15% to 50% of that tesamorelin benchmark.
That single comparison changes how the blend should be understood. Researchers discussing the stack are usually not recreating tesamorelin therapy and adding ipamorelin on top. They are often using a reduced-dose mixed system intended to probe signaling efficiency, tolerability, or practical lab handling.
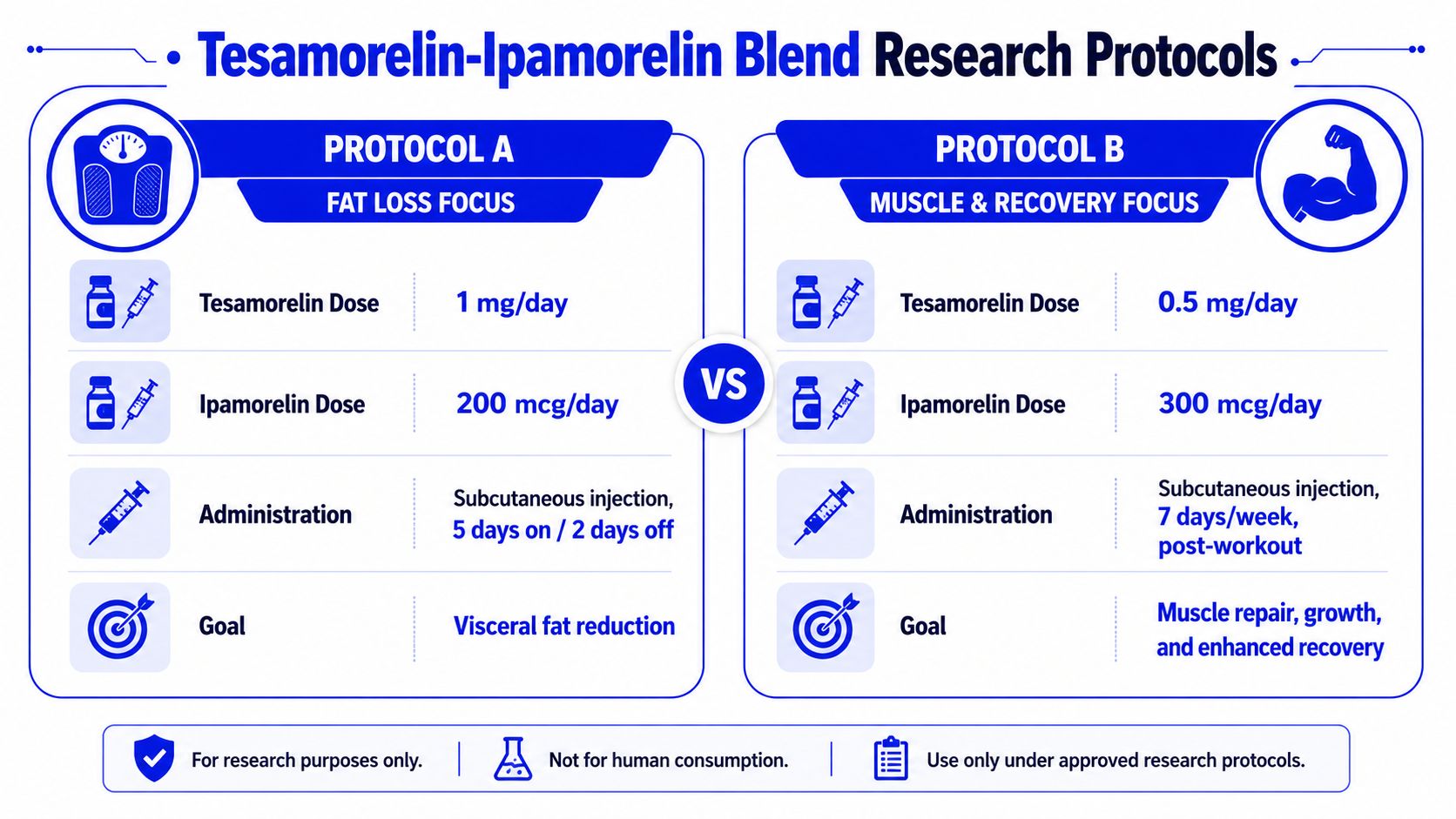
Some recurring traits show up in these research-oriented protocols:
A comparison table helps clarify the gap.
| Protocol type | Dose framework | Frequency pattern | Interpretation |
|---|---|---|---|
| FDA-labeled tesamorelin monotherapy | 2 mg once daily | Daily | Established clinical reference for tesamorelin |
| Public tesamorelin-ipamorelin blend starting approach | 300 mcg | Often daily | Research-oriented entry point |
| Public tesamorelin-ipamorelin blend escalation approach | 500 mcg or 1 mg daily | Often daily | Still below the tesamorelin monotherapy benchmark |
| Public blend cycle structure | 8–12 weeks or 5 days on, 2 days off | Intermittent cycle framing | Experimental protocol design rather than labeled therapy |
The deeper implication is easy to miss. When someone asks for a tesamorelin ipamorelin blend dosage, they may think they are asking for a stronger version of tesamorelin. The public protocol environment suggests something different: a lower-dose, mixed-signal experiment that trades standardization for theoretical synergy.
That's not a criticism. It's a design reality. If your lab treats the blend as its own category, the dosage data make much more sense.
Even a sensible protocol breaks down if the vial is prepared inconsistently. With peptide blends, handling is not a side task. Reconstitution determines whether the nominal dose on paper matches the volume that arrives in the syringe.

A commonly discussed example involves a 5 mg tesamorelin + 5 mg ipamorelin vial. The blend calculator reference describes reconstituting the 10 mg total with 3.0 mL bacteriostatic water. That produces about 3.33 mg/mL total peptide, or roughly 1.67 mg/mL of each peptide, and means each 0.1 mL corresponds to about 333 mcg total peptide.
For a technician, that last number is the operational shortcut. Once the vial is reconstituted this way, small insulin-syringe increments become easier to translate into microgram-level exposure without recalculating every draw.
A practical lab sequence looks like this:
Small-volume accuracy matters more with blends because a single draw affects two peptides at once.
Most public discussions describe once-daily subcutaneous administration, often with evening timing. That doesn't turn the practice into a standard of care. It primarily reflects the most common research handling pattern attached to the blend.
Consistency matters more than novelty here. If a protocol specifies one time window, one route, and one reconstitution standard, keep those variables stable across the run. Otherwise, you won't know whether a signal shift came from the peptides or from inconsistent preparation.
The following video offers a practical visual reference for peptide handling workflow:
Good lab practice for this category usually includes:
The main takeaway is that reconstitution isn't clerical work. It is part of the dosage itself.
A safety-first protocol is not bureaucratic overhead. It's what separates a readable result from an uninterpretable one. If a peptide blend influences the same hormonal environment that already requires monitoring in tesamorelin use, the study should assume that observation discipline matters from day one.
The clearest safety signals in this area come from tesamorelin's established labeling context and from the logic of adding a second GH-related input. Practical monitoring concerns include glucose intolerance, edema, injection-site observations, and IGF-1 tracking. Those aren't just warning labels. They are variables that can alter how you interpret efficacy, tolerability, and exposure.

A disciplined monitoring checklist often includes:
For broader background on how clinicians frame hormone-related safety questions, ProMD Health hormone therapy information can help contextualize why monitoring frameworks matter even when the compounds under discussion are being handled in a research environment.
The common mistake is treating safety controls as separate from the core experiment. They aren't. If you don't monitor the variables most likely to move, you reduce the value of any observed endpoint because you can't explain what else changed alongside it.
Good peptide research doesn't just ask whether a protocol produced a signal. It asks whether the lab can account for the conditions surrounding that signal.
This becomes more important with blends than with single agents. A combination can increase ambiguity because any response may reflect one peptide, the interaction between both, or the way the blend shifts tolerability. Careful observation doesn't remove that complexity, but it does stop the protocol from drifting into anecdote.
Researchers should also stay inside a strict compliance lane. These materials are for laboratory and research use only, not for human or veterinary consumption. That boundary should shape procurement, handling, documentation, and every communication attached to the study.
The most important fact about tesamorelin ipamorelin blend dosage isn't the syringe volume. It's the context around the number. Tesamorelin has a real dosing anchor, a regulatory history, and a clearer monitoring framework. The blend has a mechanistic rationale, public research-style protocols, and a much looser evidence base.
That creates a useful decision framework. If the research objective matches tesamorelin's documented standalone profile, a single-agent design may produce cleaner data. If the objective is dual-pathway GH signaling, then the blend becomes a hypothesis-driven tool, not a default upgrade. In either case, reconstitution accuracy, fixed administration practices, and active safety monitoring determine whether the protocol can generate interpretable results.
All content here is informational and educational only. The compounds discussed are intended strictly for laboratory and research use. They are not drugs, supplements, or products for human or veterinary consumption, and researchers must follow applicable regulations, documentation standards, and safety procedures.
If you're sourcing materials for peptide studies, Peptide Warehouse USA offers a research-focused catalog built for laboratory, analytical, and preclinical work. You can explore options, review available documentation, and learn more about their USA-made peptide supply process before planning your next protocol.



