No products in the cart.
You’re probably here because you have a vial, a syringe, a target amount, and one nagging concern: if the math is off, the whole setup is off. That concern is justified. A ghk cu dosage calculator looks simple on the surface, but the calculator only works when the inputs, unit conversions, and syringe interpretation all line up.
Most dosing mistakes don’t start with bad arithmetic. They start with assumptions that go unchecked, such as an incorrect reconstitution volume, a mislabeled target unit, or a mismatch between calculator output and the syringe in hand. For researchers comparing route-specific use cases, background reading on copper peptides for hair growth can also help clarify why concentration context matters before you ever calculate a draw.
A reliable ghk cu dosage calculator is less like a recommendation engine and more like a measurement instrument. It converts what’s printed on the vial and what you added during reconstitution into a concentration you can use. Then it converts that concentration into a draw volume that matches your research plan.
That distinction matters. A calculator can tell you how much liquid corresponds to a target amount, but it can’t fix a bad assumption upstream. If the vial strength is wrong, if the solvent volume was recorded incorrectly, or if the target amount is entered in the wrong unit, the answer looks precise while being functionally useless.
Practical rule: Treat dosage calculation as a verification process, not a convenience feature.
A sound workflow has three parts: verify the vial amount, verify the liquid volume, and verify the final pull in the syringe format you are using. Researchers who understand the underlying math don’t just get an answer faster. They catch problems before those problems affect the experiment.
A common bench error starts before the math. The vial is on the tray, the diluent has already gone in, and someone opens a ghk cu dosage calculator without confirming what was added. The calculator will still return a clean number. If the inputs are wrong, that clean number sends the whole protocol off target.

Set these four items in writing before you calculate. That habit does more for accuracy than any calculator interface.
Labs that handle injectables well treat this like any other unit-sensitive process. The same discipline shows up in dosing systems outside peptide work, including unit conversions discussed in DC experts’ Dysport Botox guide. The lesson is the same. A number is only useful if the measurement system behind it is clear.
A ghk cu dosage calculator does not verify your benchwork. It assumes the vial mass is correct, the reconstitution volume was measured correctly, and the target amount was entered in the intended unit. That is why experienced researchers pause here and audit the inputs first.
Use a short verification table before any calculation:
| Input | What to verify | Why it matters |
|---|---|---|
| Vial strength | Match the vial label to your lab notes or supplier record | Sets the total mass available in solution |
| Diluent volume | Confirm the amount actually added, not the planned amount | Determines final concentration |
| Target dose | Check mg versus mcg in the protocol | Prevents large conversion errors |
| Syringe type | Confirm the scale you will read during the draw | Prevents misreading the final volume |
One practical rule improves reproducibility fast. Write each number down at the time of reconstitution, not later.
That record is what lets you verify the calculator’s answer instead of trusting it blindly. A calculator should support the workflow, not replace basic concentration control.
A calculator gives a number. Benchwork decides whether that number is usable.
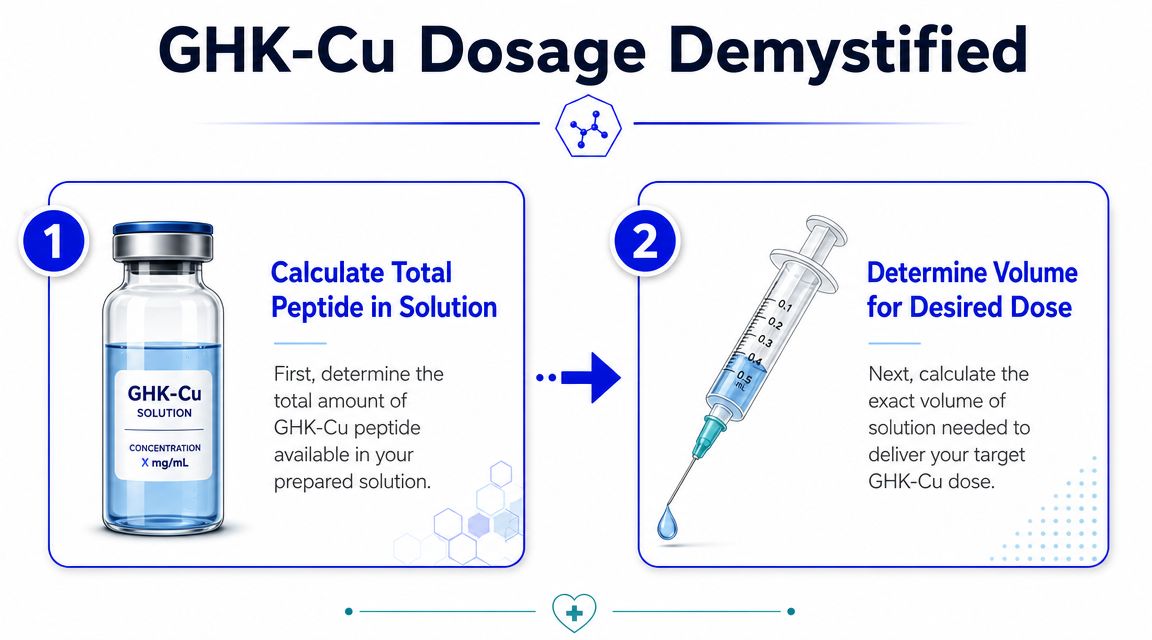
A ghk cu dosage calculator is performing two linked conversions. First, it turns vial mass and reconstitution volume into a concentration. Second, it uses that concentration to convert a target amount into a draw volume. Once you understand those two steps, you can check the output yourself instead of treating the calculator like a black box.
Start with the solution you made:
Concentration = total peptide amount ÷ total liquid volume
If a vial contains 100 mg and you add 3.0 mL of diluent, the concentration is:
100 mg ÷ 3.0 mL = 33.3 mg/mL
The same value can be written as 33,333 mcg/mL. The math did not change. Only the unit scale changed.
That distinction matters in real lab work. Protocols are often written in mcg, vial labels are often printed in mg, and syringe markings are read in mL or units. Errors usually start when one part of the calculation stays in mg and the next step shifts to mcg without a deliberate conversion.
Some researchers convert everything to mcg at the start. Others stay in mg/mL until the final step. Both methods are acceptable. The safe method is the one you can audit line by line without guessing what each number represents.
Once the concentration is known, calculate the liquid volume needed for the target amount:
Draw volume = target amount ÷ concentration
If the target is written in mcg, use concentration in mcg/mL. If the target is written in mg, use concentration in mg/mL. The units must match before you divide.
This is the point many failed calculations reveal themselves. A target amount of 500 mcg divided by a concentration written in mg/mL will give the wrong answer unless you convert one side first. The arithmetic can look clean and still be wrong on the bench.
Bench note: If the final draw volume looks unusually large or too small to measure cleanly, stop and recheck the units before you touch the syringe.
Syringe markings add one more translation layer. On a U-100 insulin syringe, 1 unit = 0.01 mL. That means a calculated volume of 0.05 mL corresponds to 5 units, and 0.10 mL corresponds to 10 units.
This is where practical handling matters. A mathematically correct draw may still be a poor setup if the volume lands between markings or is small enough to increase reading error. In those cases, researchers often adjust the reconstitution volume ahead of time so the final pull is easier to measure with the syringe on hand.
Confusion over “units” is not unique to peptide work. The same measurement problem shows up in other dosing systems, which is why DC experts’ Dysport Botox guide is a useful reminder that a unit only has meaning inside the correct product and measurement standard.
The practical takeaway is simple. The formula is not hard, but it is unforgiving. If you can explain how mass became concentration, and how concentration became volume, you can verify the calculator’s answer before it becomes a dosing error.
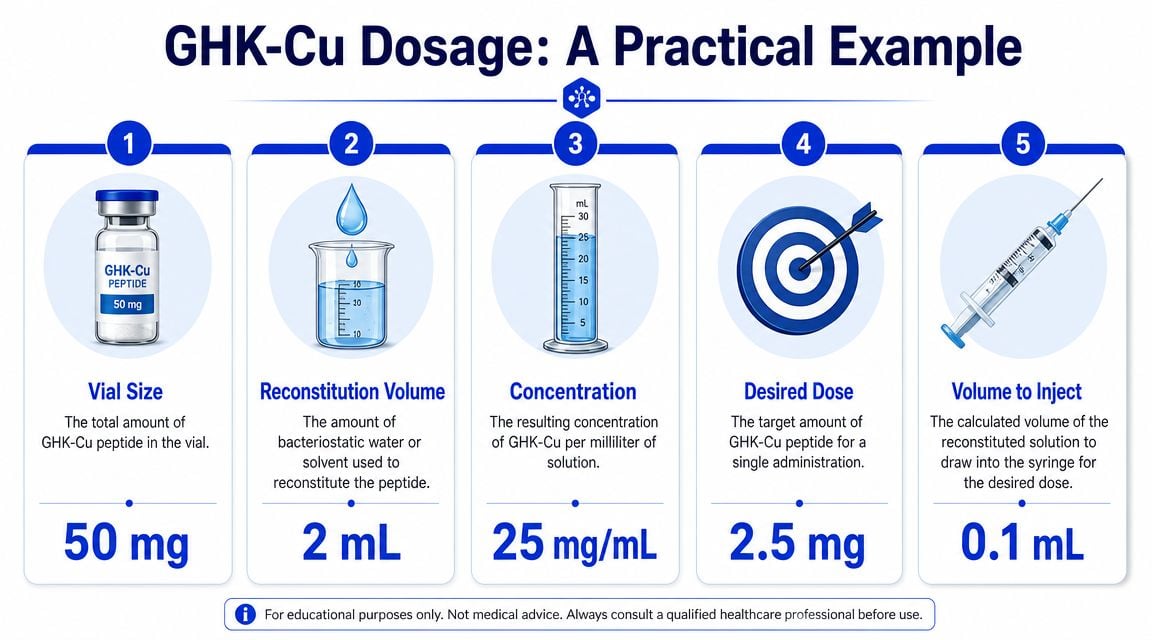
Theory matters, but confidence comes from doing the math on a complete example. Use a vial that contains 50 mg of GHK-Cu, reconstitute it with 2 mL, and set a target amount of 1 mg for the draw.
Start with the total mass and total liquid:
Use the concentration formula:
Concentration = total amount ÷ total liquid
So:
50 mg ÷ 2 mL = 25 mg/mL
That means every 1 mL of the solution contains 25 mg of GHK-Cu.
If you prefer to visualize it another way, each 0.1 mL contains one-tenth of that amount. That gives you a quick sense of whether the final draw volume should be large, small, or barely measurable.
Now apply the target amount:
Use the second formula:
Draw volume = target amount ÷ concentration
So:
1 mg ÷ 25 mg/mL = 0.04 mL
That’s the volume required to deliver 1 mg from this particular solution.
A quick cross-check helps. If 1 mL contains 25 mg, then 0.04 mL should contain 1/25 of that mL amount. The relationship makes sense. This is the sort of mental check that catches keyboard-entry mistakes before they turn into handling mistakes.
Write the result in both forms immediately: 0.04 mL and its syringe equivalent.
On a U-100 insulin syringe:
So:
0.04 mL × 100 = 4 units
The final draw for this worked example is 4 units on a U-100 syringe.
Here’s the same example in a compact table for bench use:
| Variable | Value |
|---|---|
| Vial amount | 50 mg |
| Reconstitution volume | 2 mL |
| Final concentration | 25 mg/mL |
| Target amount | 1 mg |
| Draw volume | 0.04 mL |
| U-100 equivalent | 4 units |
This example also shows why understanding the process matters more than memorizing a number. Change the reconstitution volume and the concentration changes. Change the concentration and the unit pull changes with it. The calculator is only correct for the exact setup entered into it.
Some of the worst dosing mistakes happen after the math is technically complete. The calculation may be right, but the handling between notebook and syringe introduces distortion.

Practical accuracy issues often come from rounding errors, unit confusion between mg, mcg, and IU, or changes in diluent volume after the calculation has already been generated, as discussed in this video on peptide dosing accuracy. The same source also notes that calculators may output syringe pull distances and insulin-unit equivalents, but they don’t account for the precision limits of common low-volume syringes, where a small error becomes material at very low doses.
That point matters more than most users realize. Two people can use the same ghk cu dosage calculator correctly and still end up with different practical results because vial strength, reconstitution volume, and syringe calibration differ.
The common failure points are usually these:
If the target volume is extremely small, the measurement challenge may become more important than the math itself.
A visual refresher can help when translating calculation into handling technique.
In a lab setting, the safest habit is a double-entry check. Record the target amount, convert it once, then confirm the answer in both mL and U-100 units before drawing.
Use this workflow every time:
That last step is often skipped. It shouldn’t be. A mathematically valid answer can still be awkward to execute if the draw lands in a range where tiny reading differences matter too much for your setup.
A calculator gives you a draw volume. It does not set the protocol. That separation matters because GHK-Cu appears in multiple research and product contexts, and each context uses different concentration logic.
A common weakness in many ghk cu dosage calculator pages is that they stop at mg-to-mL conversion. In practice, that is only part of the job. GHK-Cu is discussed across categories with very different concentration ranges, including 2% to 10% for topicals and 0.1% to 1.0% for injectables, as described in Neurogan Health’s overview of GHK-Cu dosage contexts.
That difference changes the entire calculation question. A topical concentration is a formulation problem. An injectable target is a reconstitution and draw-volume problem. If you treat those as interchangeable, the math may look clean while the setup is wrong.
This is why protocol context has to come first.
The GHK-Cu 100 mg vial dosage protocol page describes a 1 mg/day phase followed by 2 mg/day, often using a 100 mg vial reconstituted with 3.0 mL. In that setup, 1 mg corresponds to about 4 U-100 units, and 2 mg corresponds to about 8 U-100 units. The same page also outlines a broader 1 to 2 mg daily range, often on a 5-days-on/2-days-off pattern over 8 to 12 weeks, plus another schedule of 1.0 to 2.0 mg daily for 30 to 60 days on followed by 30 to 60 days off, and a lower 0.5 to 1.5 mg daily or every other day range.
Those examples show variation in protocol design, not a single standard you can apply blindly. A calculator cannot tell you which schedule fits the research objective, preparation type, or route. It can only convert the selected target into a measurable volume based on the vial amount and the exact liquid added during reconstitution.
That underlying principle matters more than the tool itself. Once you understand concentration, you can audit the calculator output instead of trusting it by habit. If the protocol calls for 1 mg, but the reconstitution volume was changed from the assumed setup, the syringe units must change too. That is how researchers avoid copying a number from a reference page into a completely different vial condition.
A protocol defines the target. The calculator verifies how to measure it.
Researchers get more reliable results when they treat calculation as a verification step inside the protocol, not as a substitute for protocol design.
Accurate peptide work depends on disciplined handling more than fast math. A ghk cu dosage calculator is useful because it translates vial mass and reconstitution volume into a draw you can measure, but it only performs well when every input is verified. That’s why careful researchers check the vial amount, confirm the exact liquid volume, keep units consistent, and cross-check the final result in both mL and syringe markings.
The practical edge comes from understanding the logic behind the output. When you know how concentration and draw volume are derived, you can audit the result, spot bad assumptions, and protect the reproducibility of your work. All information here is educational only. Products such as GHK-Cu are for laboratory and research use only, not for human consumption.
For researchers who want a dependable supply chain before they even open the calculator, Peptide Warehouse USA offers high-purity, USA-manufactured research peptides with third-party documentation, batch testing, and clear research-use positioning. Learn more and explore options for your next lab project.



