No products in the cart.

You're probably staring at a vial, a syringe, and a calculator tab, double-checking the same numbers because one small mistake changes the whole concentration. That's a normal place to be. HGH reconstitution looks simple until you have to convert IU, milliliters, and syringe units into one clean, repeatable draw.
An accurate HGH reconstitution calculator removes a lot of that friction, but its primary advantage isn't convenience. It's understanding why the math works, so you can catch bad assumptions before they affect your research. Once you understand IU vs mg, how diluent changes concentration, and where handling errors happen, you're no longer copying a formula. You're controlling the procedure.
The biggest source of confusion in HGH work is that the vial doesn't behave like many other peptides. With compounds such as BPC-157 or GHK-Cu, people often think in mass. HGH adds another layer because the reference system is based on biological activity.
Human Growth Hormone is measured in international units rather than micrograms, and the accepted standard for high-purity recombinant HGH is 1 mg ≈ 3 IU according to the World Health Organization-based reference described here. That single conversion is the foundation of any reliable HGH reconstitution calculator.

If you skip that distinction, the rest of the math gets shaky fast. A vial labeled in IU tells you about standardized activity, not just mass alone. That's why researchers who are comfortable reconstituting mass-based peptides can still get tripped up by HGH.
A calculator isn't just dividing volume by dose. It's translating the vial content into a concentration you can measure on a syringe. The HGH calculator reference notes that the globally accepted standard is approximately 1 mg equaling 3 IU, and that this fixed ratio is what allows vial sizes such as 10 IU, 12 IU, or 36 IU to be translated into practical syringe units.
Practical rule: If the IU-to-mg relationship is wrong at the start, every later draw is wrong even if your syringe reading is perfect.
That's the “why” behind reconstitution. You aren't just dissolving powder. You're creating a known concentration that lets one measured liquid volume correspond to one intended amount of HGH activity.
A few ideas keep the whole system straight:
Once those three ideas click, the calculator stops feeling like a black box. It becomes a shortcut for math you understand well enough to verify.
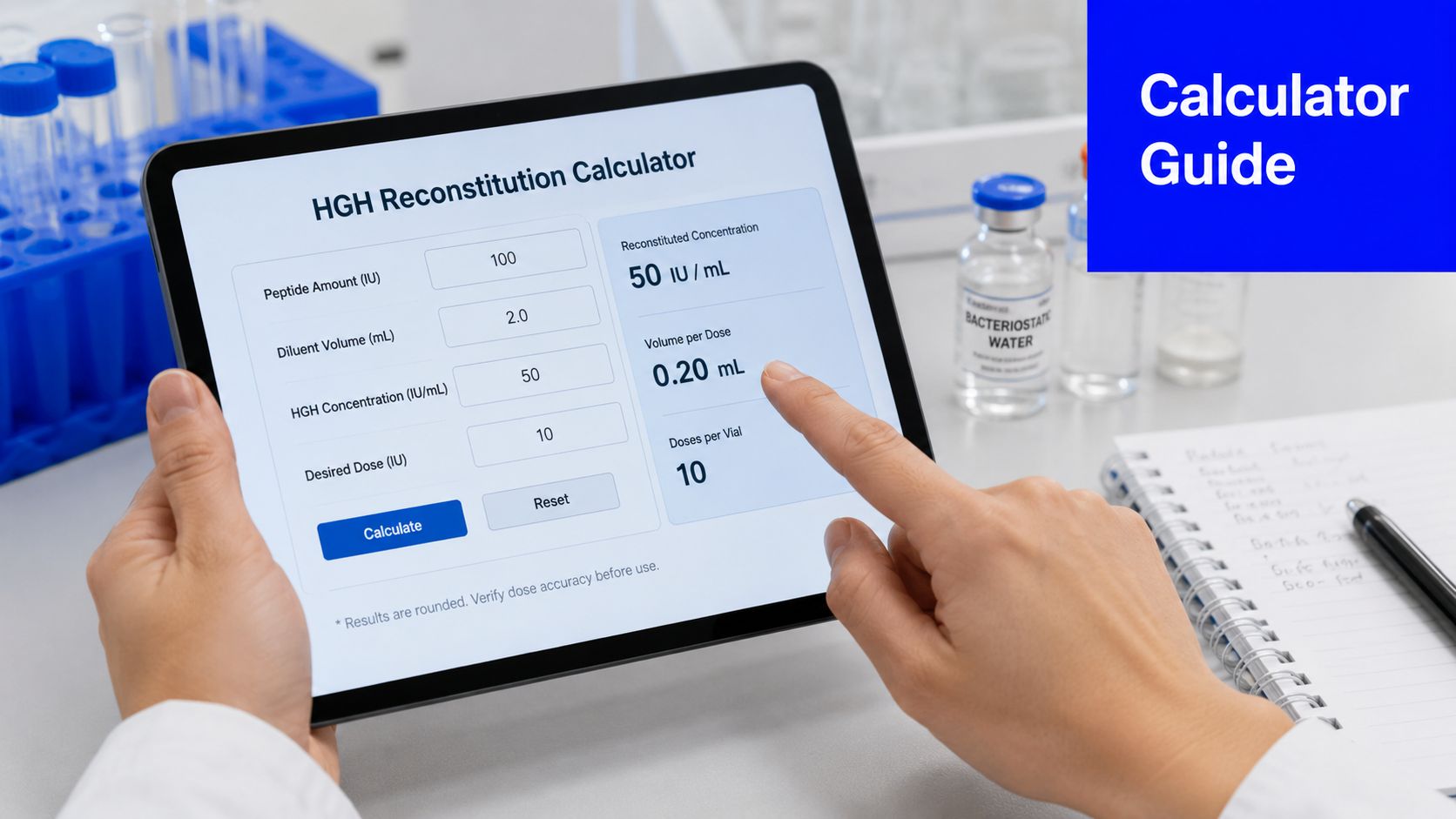
A good HGH reconstitution calculator is simple on the surface. You enter what's in the vial, you enter how much bacteriostatic water you add, and the tool returns a concentration and draw amount.
The core input fields are straightforward. An HGH reconstitution calculator overview explains that the tool needs the total amount of HGH in the vial in IU and the volume of diluent added in mL, then calculates the final IU per mL concentration and the exact volume to draw for a chosen IU dose.
That means the calculator is only as accurate as the values you enter. If you misread the vial strength or type the wrong water volume, the output can still look neat and precise while being wrong.
Most tools return two useful outputs:
Some researchers mentally jump straight to syringe units. That's workable, but concentration should come first. When you know the concentration, you can sanity-check any later number the calculator shows.
Read the result in order. First ask, “What concentration did I create?” Then ask, “What liquid volume gives my target dose?”
Take a conceptual example. If a vial contains 10 IU and you add 1 mL of bacteriostatic water, your concentration becomes 10 IU per mL. If your target is 2 IU, you'd draw 0.2 mL.
On a standard U-100 insulin syringe, 1 mL equals 100 units, which means 0.2 mL equals 20 syringe units. That final conversion is where many people get lost, but it's only a volume conversion after concentration has already been established.
Use this sequence every time:
This approach also helps when you're using non-standard concentrations. You don't need to memorize every scenario. You just need to trust the sequence and verify the concentration before drawing anything.
A calculator can give a clean number, but the vial only contains that concentration if the liquid volume and handling are correct. In practice, reconstitution is where the math becomes a physical solution. Small bench errors change the concentration you think you made, and that changes every dose drawn afterward.
Start with a simple scenario. You plan to add 1 mL of bacteriostatic water, but a rushed setup leads to an air bubble, a partial draw, or an interrupted transfer. The calculator still assumes 1 mL. Your vial does not.
That is why setup matters. Reconstitution is measurement first, mixing second.
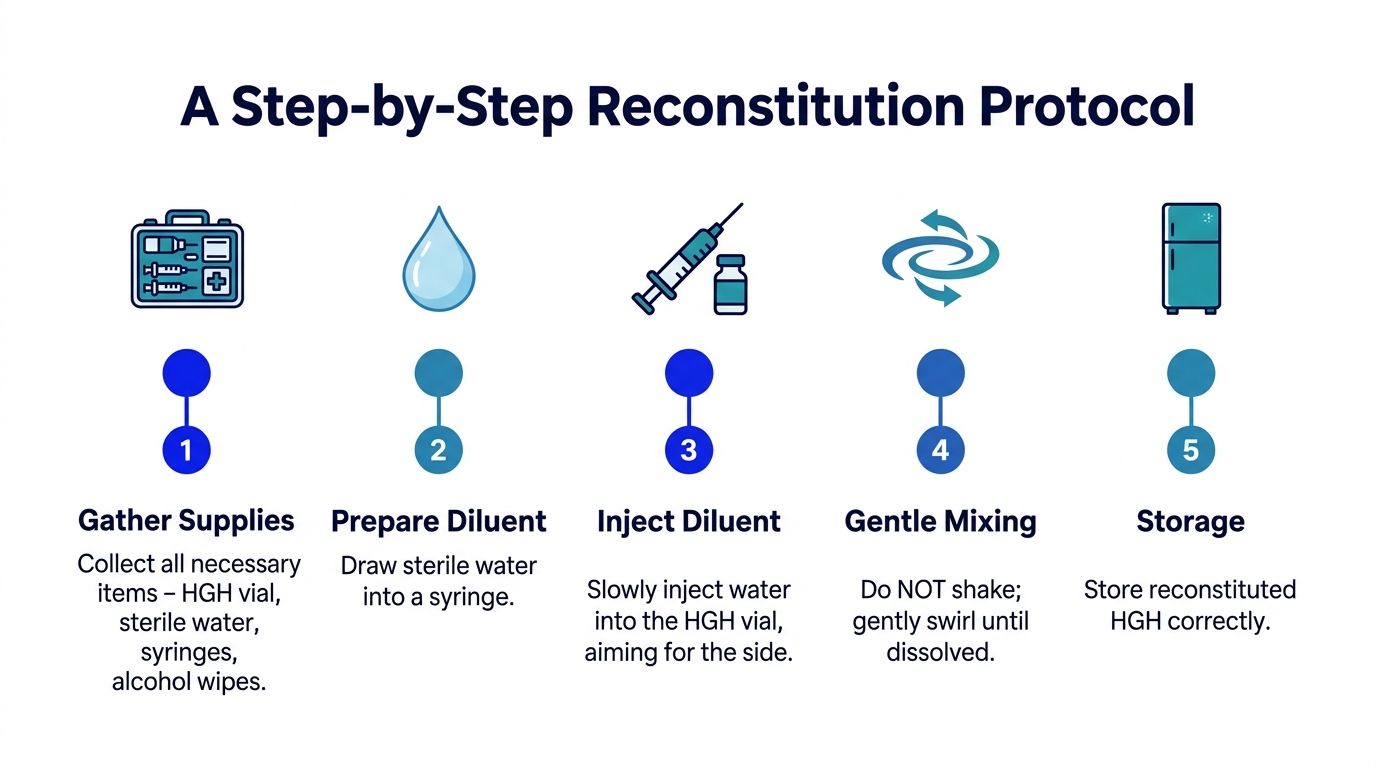
Keep the vial, bacteriostatic water, syringe, and alcohol wipes together before you begin. A prepared bench reduces handling mistakes and helps you focus on the one variable that controls concentration at this stage: the exact volume of diluent added.
For a commonly used benchmark, the standard 10 IU HGH protocol described here uses exactly 1 mL of bacteriostatic water and notes that this setup achieves a final concentration of 5.00 mg/mL, simplifying syringe readability. The same source also states that, in this setup, the solution yields 7 doses per vial when the target dose is approximately 26.5 units (0.266 mL), and that a standard U-100 syringe treats 1 mL as 100 units.
Use examples like that as calibration, not as a rule to copy blindly. The lesson is the relationship between vial content and diluent volume. Change either one, and the concentration changes with it.
The powder should dissolve gently. Direct pressure from a fast stream can disturb the cake and make the process harder to control.
Use this sequence:
That wall-first approach works like rinsing the side of a beaker instead of blasting the material at the bottom. The goal is controlled wetting across the powder, which helps preserve handling consistency and makes the final volume easier to trust.
Meniscus reading matters here too. Read the liquid at eye level so the measured volume matches the volume entered into the calculator. A small misread at the syringe becomes a concentration error in the vial.
Here's a visual reference for the process:
After the diluent is in the vial, give the solution time to dissolve. Gentle swirling is fine. Vigorous shaking can damage peptide integrity.
This step often confuses researchers because the vial may look inactive for a moment. That pause is normal. Dissolution is not improved by rough handling.
Before drawing any amount, inspect the solution. You want a clear, fully dissolved mixture with no visible particles or dry material left on the glass. If material remains, wait and use light swirling again.
A short bench checklist helps:
Slow, deliberate technique protects the logic behind the calculator. If the math says one thing and the bench work produces another, the bench result is the one that determines the dose.
Examples are where the process usually clicks. Once you see the same math applied to more than one vial size, you stop treating the calculator as a mystery tool and start using it as a verification tool.
Start with a 10 IU vial and add 1 mL of bacteriostatic water. The final concentration is 10 IU/mL.
If the target dose is 2 IU, divide the target dose by the concentration:
On a U-100 insulin syringe, 0.2 mL corresponds to 20 units. This is a clean example because the concentration makes the conversion easy to visualize.
If your concentration is 10 IU per mL, every 0.1 mL contains 1 IU. That mental shortcut makes quick bench checks much easier.
Now use a 36 IU vial and add 2 mL of bacteriostatic water. The concentration becomes 18 IU/mL.
For a 2 IU dose:
On a U-100 syringe, that works out to about 11.1 units. For this reason, calculators become especially useful, because larger or less convenient vial sizes often produce awkward draw volumes that aren't easy to estimate mentally.
A 12 IU vial with 2 mL of water gives another useful comparison. That concentration is 6 IU/mL, so a 2 IU dose would require:
That equals about 33.3 units on a U-100 syringe.
| Vial Size (IU) | Bacteriostatic Water (mL) | Final Concentration (IU/mL) | Volume for 2 IU Dose (mL) | Syringe Units (on U-100) |
|---|---|---|---|---|
| 10 | 1 | 10 | 0.2 | 20 |
| 12 | 2 | 6 | 0.333… | 33.3 |
| 36 | 2 | 18 | 0.111… | 11.1 |
A few patterns stand out:
When researchers ask how much water they should add, they're often really asking a different question. They want a concentration that makes the syringe readable and repeatable for the doses they plan to test.
A dosing error often starts with a number that looks harmless. The vial says IU. The calculator asks for mL. The syringe shows units. If those labels are treated as interchangeable instead of related, the final draw can be wrong even when each step feels reasonable.
That is why good practice starts before the syringe touches the vial. Reconstitution is a concentration problem first and a handling problem second. You are deciding how much HGH is present in each milliliter, then translating that concentration into a measurable draw. If either part is off, the dose is off.
The first failure point is unit confusion. IU describes biological activity. mL describes liquid volume. Syringe units on a U-100 insulin syringe describe fractions of a milliliter. They are connected, but they are not the same thing. Treating them as the same is like confusing the amount of solute in a beaker with the size of the beaker itself.
A second problem is input error. Entering the wrong vial strength, selecting the wrong diluent volume, or forgetting to convert the final mL draw into syringe units can shift the result enough to affect repeatability. As noted earlier, simple reconstitution volumes such as 1 mL or 2 mL are common partly because they make the concentration easier to check mentally. Once the mixture becomes more dilute, the draw volume gets larger, and small reading errors become easier to make.
One practical rule helps here. Before drawing anything, say the concentration out loud in plain language: "This vial now contains X IU per mL." That sentence forces the math into a form you can verify.
A correct calculation can still fail at the bench. If the diluent is pushed directly onto the powder with force, if the vial is shaken aggressively, or if the plunger is read from above instead of straight on, physical technique adds variability after the calculator has already done its job.

Read the syringe at eye level. That reduces parallax error, which is the same visual problem that makes a meniscus look different when viewed from an angle. On a small draw, a tiny misread matters more than researchers expect.
The choice of diluent volume matters for the same reason. More water does not change the total IU in the vial. It changes how spread out those IU are. A dilute mixture may be easier to dissolve, but it also means larger draw volumes. A concentrated mixture gives smaller draws, but those draws may land between syringe markings and become harder to reproduce. The best setup is usually the one that gives a clean, readable measurement for the doses you plan to use.
Accurate dosing depends on two translations done correctly: total IU into IU per mL, then IU per mL into a syringe volume you can read consistently.
Use the same small checklist every time:
Consistency comes from reducing opportunities for drift. The fewer judgment calls you leave for the moment of dosing, the more reliable the process becomes.
The basic calculator gets you a concentration. It doesn't always tell you whether that concentration is practical for the full life of the vial, or whether your storage window supports the way you plan to use it.
An HGH stability discussion notes that HGH in bacteriostatic water typically requires storage at 2-8°C and use within 30-56 days. That same source also points out that many calculators don't actively track this stability window.
A broader peptide handling reference on storage and stability states that reconstituted peptide solutions remain stable for 3 or more weeks at +4°C and 3–4 months at -20°C, while repeated freeze-thaw cycles should be avoided. That doesn't replace batch-specific handling judgment, but it does reinforce the importance of time and temperature.
Many users focus only on “What draw gives my dose?” The more useful question is often “What concentration gives me accurate draws without keeping the vial reconstituted longer than I want?”
That's especially relevant when someone tries to create a non-standard concentration such as a neat round IU-per-mL target. A calculator can solve the math, but it usually won't tell you whether that choice creates awkward storage timing for your protocol.
Can I use any water volume I want?
Mathematically, yes, if the calculator accounts for it. Practically, readability and stability both matter.
Why do some setups feel easier to dose than others?
Because concentration determines whether your target draw lands on clear syringe markings or awkward fractions.
Should I freeze and thaw repeatedly?
No. Repeated freeze-thaw cycles should be avoided to preserve peptide integrity, as noted in the storage reference above.
Why aren't all calculators enough on their own?
Because many handle concentration well but don't manage batch-specific storage windows or workflow decisions around usability.
If you're sourcing research-grade compounds and want a supplier focused on traceability, batch testing, and clear documentation for laboratory use, explore Peptide Warehouse USA. You can learn more about their catalog, review available research products, and explore options that support organized, consistent peptide research workflows.




Leave a comment