No products in the cart.

Are peptides changing fat biology, or are many researchers just observing better appetite control and calling it “fat burning”?
That gap matters. Discussions about peptide therapy for fat loss often blur three very different things: receptor pharmacology, clinical outcomes, and commercial hype. If you’re evaluating these compounds in a laboratory, those categories can’t be mixed. A mechanism is not a guarantee of a body-composition outcome, and a body-composition outcome is not proof that every tissue compartment responded the same way.
A careful research view is more useful. Some peptide classes have meaningful human data. Others are still best treated as exploratory tools for pathway analysis, signal mapping, or preclinical model work. The most credible findings come from studies that pair peptide exposure with controlled nutrition, behavior, and proper endpoint selection, not from vague claims about “melting fat.”
Research interest remains high because the field touches several metabolic control points at once. As one overview notes, peptide therapy for weight loss has been described as more gradual and more systemic in its metabolic effects, with observed changes in energy, digestion, and body composition often appearing within 6 to 12 weeks when combined with proper nutrition and exercise (reviewed here). For research use only, that makes peptides valuable not as miracle compounds, but as probes of satiety signaling, glucose handling, gastric emptying, and tissue-level adaptation.
Peptides are short amino acid sequences that can interact with highly specific biological targets. In fat loss research, that specificity is the reason they matter. A peptide may influence appetite signaling, insulin dynamics, gastric emptying, or neuroendocrine communication, all of which can alter body mass trajectories under controlled conditions.
For a scientist, the phrase peptide therapy for fat loss should trigger caution before enthusiasm. The first question isn’t “Does it work?” but “What exactly changed?” Reduced food intake, altered substrate use, slower gastric transit, improved insulin sensitivity, and changed body composition can overlap, but they aren’t interchangeable findings.
A useful way to think about peptide research is to separate the field into two layers:
That distinction keeps studies honest.
Working principle: A peptide is scientifically interesting only when the mechanism, exposure conditions, and measured outcomes line up.
Laboratories also need to keep the regulatory context clear. Research peptides are not consumer wellness products in this setting. They are reagents or investigational compounds used in analytical, in vitro, and preclinical workflows. That means formulation quality, lot consistency, storage, and assay design often matter as much as the compound identity itself.
Confusion usually starts when readers assume all peptides in this space do the same thing. They don’t. Some are studied because they mimic endogenous hormones. Others are explored because they may influence growth hormone pathways, energy partitioning, or recovery-related processes that indirectly affect body composition. The evidence is strongest where receptor biology is well defined and human trials are available.
How does a peptide change fat metabolism in a study setting? The short answer is that it usually changes regulation first, then body composition later. For research use only, that distinction matters because a shift in fat mass can arise from several upstream processes that look similar at the scale of body weight.
Most peptides studied in metabolic research act through receptors already involved in appetite control, glucose handling, gastric motility, or energy balance. A receptor works like a molecular switchboard. Once a peptide binds, intracellular signaling changes, and those changes can alter feeding behavior, hormone release, and nutrient flow between tissues.
GLP-1 receptor agonism is one of the clearest examples because the pathway itself is well characterized. Investigators study this axis because it links the gut, pancreas, brain, and gastrointestinal tract in a measurable way. In that context, reduced intake is often the first observable effect, while changes in fat mass appear later and must be interpreted alongside lean mass, activity, and total energy intake.
A visual summary helps clarify the main pathways under investigation:
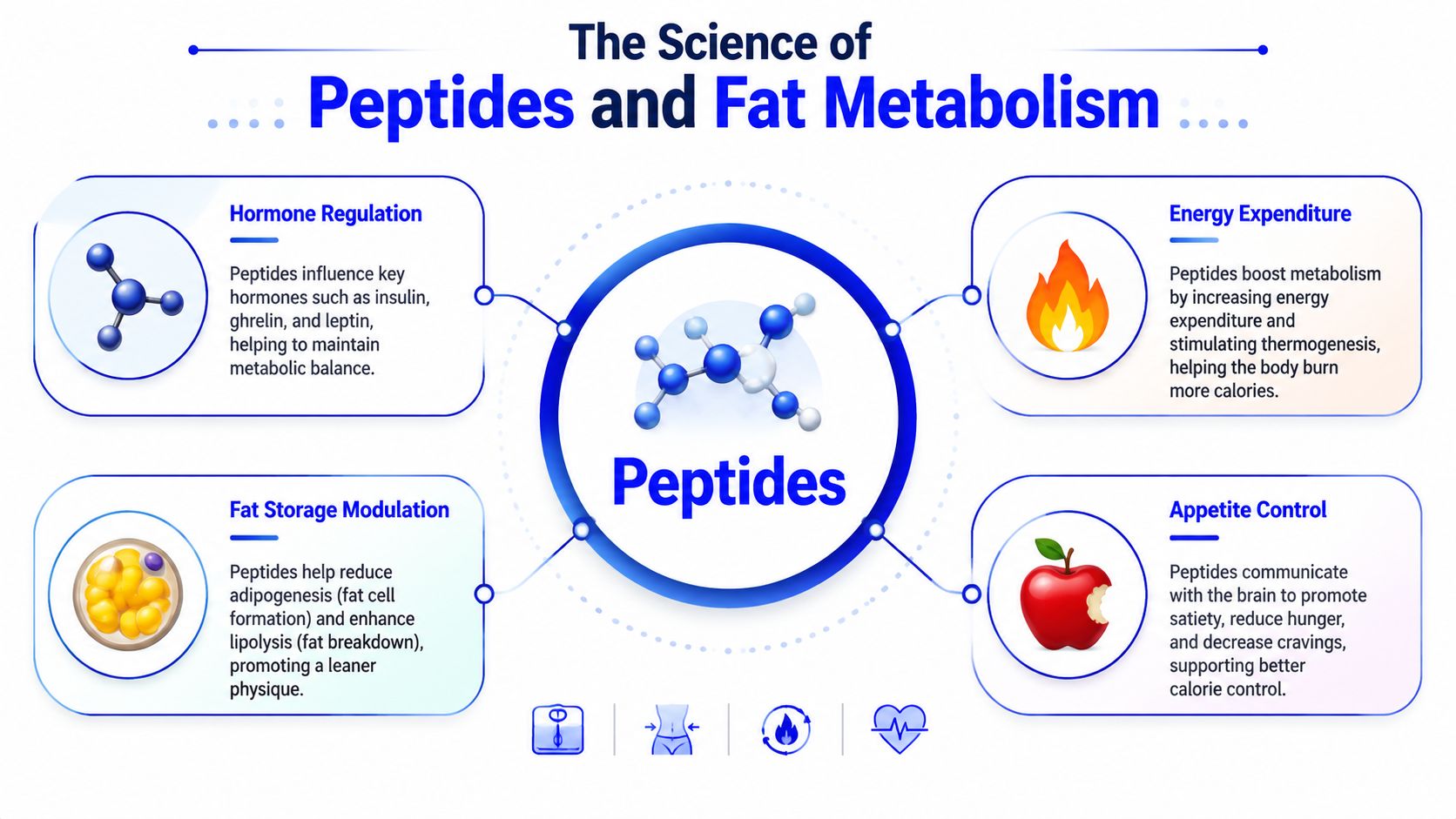
Researchers usually separate peptide effects into three mechanistic buckets, even though real studies often show overlap.
Appetite regulation
Some peptides change hunger signaling, satiety, meal size, or the rate at which the stomach empties. In practical terms, that can reduce caloric intake without any direct demonstration that adipose tissue oxidation increased.
Hormonal coordination
Peptides can shift endocrine timing and signal strength, especially in pathways tied to insulin and glucagon. That matters because nutrient partitioning determines whether incoming energy is stored, oxidized, or used to preserve lean tissue.
Energy expenditure and substrate handling
A smaller group of claims concerns lipolysis, thermogenesis, and fuel selection. In such cases, careful interpretation is required. A study may report lower fat mass, but unless the protocol directly measured substrate oxidation, calorimetry, or body composition, the mechanism remains partly inferred.
A lower body weight endpoint does not identify the cause. Researchers need to separate reduced intake, fluid loss, altered fuel use, and changes in lean mass.
That separation is especially important in GLP-1 related study design. Investigators interested in optimizing GLP-1 weight loss results often focus on preserving muscle and controlling for exercise, since those variables can change how body composition data should be interpreted.
The section below expands on this visually and conceptually:
This is a common point of confusion. If a peptide increases satiety and fat mass later declines, the study supports an effect on energy balance. It does not automatically prove a direct adipocyte-level action.
A useful analogy is to compare metabolism research to tracing flow through a plumbing system. The reading at the outlet may change, but that does not tell you which upstream valve moved unless each segment was measured. In peptide studies, those segments include food intake, gastric emptying, insulin dynamics, physical activity, lean mass retention, and direct markers of substrate use.
For that reason, careful papers avoid broad consumer language such as “fat-burning peptide.” In a research-only framework, stronger wording is reserved for situations where the experimental design directly tested the pathway being claimed.
Which peptides have human evidence that can support a fat loss hypothesis, and which are still better treated as exploratory tools? That distinction matters because receptor plausibility, online discussion, and actual clinical outcomes are three different categories of evidence.
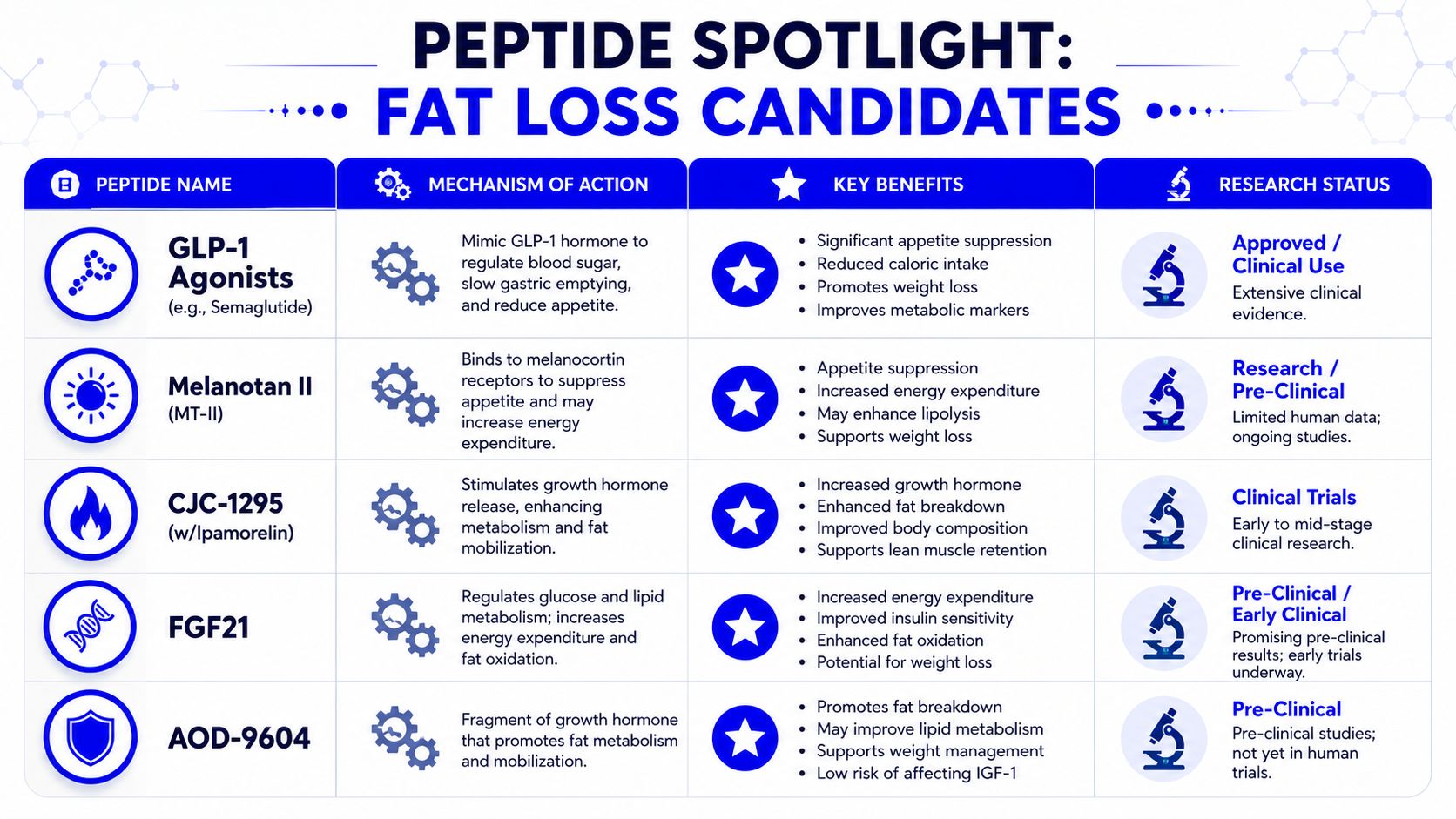
For research use only, the most defensible starting point is to sort peptides by evidence tier. One tier includes agents studied in large human trials with defined receptor targets and prespecified clinical endpoints. Another includes compounds discussed because their pathway logic is interesting, even though direct fat loss evidence remains limited. Mixing those tiers leads to weak conclusions.
Semaglutide sits in the highest-evidence group because investigators can connect mechanism, dose exposure, and long-term human outcomes through a relatively clear chain of evidence. The strongest support concerns body weight reduction under controlled clinical conditions, usually alongside dietary and behavioral support, rather than direct proof of selective adipocyte destruction.
Mechanistically, semaglutide acts through the GLP-1 receptor. In study settings, that makes it useful for examining satiety signaling, meal size, gastric emptying, and downstream changes in energy intake. A plumbing analogy helps here. If water flow falls at the outlet, the immediate question is whether the valve changed upstream, the pipe narrowed, or less water entered the system. With semaglutide, reduced body weight can reflect altered intake behavior and metabolic regulation, but the design has to measure those steps if the paper wants to claim them.
For that reason, semaglutide is best described as a peptide-based research tool for studying appetite-linked body weight change. It should not be presented as proof that any GLP-1 pathway compound directly “burns fat” in isolation.
Tirzepatide is also supported by formal human data, but its scientific interest comes from more than the size of the observed effect. It engages multiple incretin-related signaling pathways, which gives researchers a way to study how combined receptor activity can alter food intake, glycemic control, and body composition over long intervals.
A careful interpretation stays narrow. If a trial reports a substantial reduction in body weight over many months, that finding supports a sustained effect on whole-body energy balance under the tested conditions. It does not settle the separate question of how much of that change came from fat mass versus lean mass unless the protocol measured body composition directly.
That point is easy to miss. Large weight changes can make a peptide look mechanistically simpler than it is.
In laboratory planning, tirzepatide fits studies that need a comparator for dual-pathway signaling, especially when the protocol includes food intake records, DEXA or similar body composition methods, and prespecified rules for interpreting lean tissue changes.
Compounds such as CJC-1295, Ipamorelin, and AOD-9604 appear often in catalogs and discussion forums because the growth hormone axis has plausible links to body composition. Researchers may ask whether changes in pulsatile growth hormone signaling, recovery physiology, or nutrient partitioning could indirectly affect fat mass.
The problem is evidence depth. Compared with GLP-1 related agents, these peptides have much less human outcome data for fat loss endpoints.
That does not make them irrelevant for research use. It places them in a different bucket. A graduate student designing a study should treat them as hypothesis-generating compounds unless there is a tightly defined rationale, such as testing a specific endocrine pathway, a kinetic question, or a preclinical model with a clear mechanistic readout.
The practical sorting logic looks like this:
| Research question | Better fit |
|---|---|
| Appetite regulation and feeding behavior | GLP-1 pathway compounds |
| Dual-pathway effects on body weight regulation | Tirzepatide-related models |
| Growth hormone axis signaling | CJC-1295 or Ipamorelin models |
| Indirect body composition hypotheses with limited clinical backing | AOD-9604 or similar exploratory compounds |
Some peptides gain attention from anti-aging, performance, or recovery communities before they gain support in controlled obesity or body composition research. That pattern is common, but it creates a sourcing and interpretation problem. A reagent can be popular long before it is well characterized for the endpoint being studied.
In that setting, quality control becomes part of scientific reasoning, not just purchasing. Laboratories should verify identity, purity, lot consistency, storage requirements, and vendor documentation before assigning biological meaning to a result. Researchers familiar with supplement testing language may find some overlap in quality-assurance concepts discussed in understanding NSF certified supplements, although peptide reagents for laboratory use require their own analytical standards and documentation.
A useful rule is simple. The stronger the claim, the stronger the evidence chain must be.
For research use only, peptides with established human trial programs should anchor confirmatory work. Peptides with thinner evidence can still be worth studying, but only when the protocol states exactly which mechanism is being tested and which measurements would falsify the hypothesis.
What does a fat-loss peptide study measure if the vial contains the wrong sequence, a degraded product, or a mixture of impurities?
Poor reagent quality can break the chain of inference before the experiment even begins. A change in body weight, glucose handling, food intake, or lipid markers may look like a peptide effect, but the signal may come from contamination, oxidation, aggregation, concentration error, or simple mislabeling. In research use only settings, that distinction matters because mechanism claims are only as credible as the material used to test them.

Peptide quality works like calibration in analytical chemistry. If the reference material is wrong, every downstream readout becomes harder to interpret. A study can still produce a statistically significant result, but significance does not identify the active species in the vial.
That problem becomes more serious in peptide research because many compounds in this field are discussed with unusually strong expectations. Some have controlled clinical data behind them. Others are supported mainly by mechanistic reasoning, animal work, or anecdotal discussion. Those evidence tiers should not be treated as interchangeable. If a laboratory starts with a low-confidence reagent and a high-expectation hypothesis, confirmation bias becomes easier to miss.
Purity is only one variable. Identity, counterion content, residual solvents, peptide truncations, oxidation products, and endotoxin burden can all alter biological behavior. For example, an inflammatory response caused by contamination can change feeding behavior or metabolic readouts and be mistaken for pathway-specific activity. In that case, the experiment has generated noise with a biological costume.
Laboratories should document several checks before a peptide enters any protocol.
A practical comparison helps here. Researchers would not accept an antibody with no validation history and then make a strong claim about receptor expression from a single blot. Peptides deserve the same skepticism. Sequence-dependent biology cannot be interpreted well when the reagent itself is poorly characterized.
Lab rule: If you would not trust the material in assay validation, do not trust it in a body-composition study.
Sourcing also deserves more scrutiny than many peptide articles allow. Marketing terms such as “research grade” or “high purity” have little value without lot-specific documentation. A serious supplier should provide analytical records, storage guidance, and a clear statement of intended research use. If those records are vague, missing, or recycled across lots, the purchasing decision is already affecting study quality.
Cross-laboratory reproducibility often fails here first. Two groups may report results for the same named peptide while working with different impurity profiles, different actual concentrations, or different degradation states. The disagreement may look biological. The simpler explanation is often procurement and handling.
For research use only, quality assurance is not a purchasing detail. It is part of causal inference.
What separates a legitimate research peptide from a product marketed with scientific language but little regulatory substance?
The answer starts with category. A peptide used in a laboratory study sits in a different legal and scientific class than an approved drug product. That difference affects procurement, recordkeeping, ethics review, storage, labeling, and the strength of any claim a researcher can make from the results. In fat loss research, confusion at this step often creates bigger problems than receptor biology or study design.
Peptides sold for research are generally intended for analytical work, cell studies, or preclinical investigation. They are not interchangeable with finished pharmaceuticals manufactured under drug approval standards. A vial label, a purity claim, or a vendor’s marketing language does not change that status.
A useful comparison comes from third-party verification discussions outside the peptide field. The article on understanding NSF certified supplements shows why certification language, product quality language, and regulatory status need to be kept separate. The same logic applies here. A material can be described as tested and still lack the documentation needed for defensible laboratory use. It can also be analytically characterized without being approved for clinical administration.
That distinction matters because “research grade” is a supplier description, not a regulatory category with uniform legal meaning. For a scientist, the practical question is narrower. What evidence shows that the material in the tube is the material named on the label, at the stated concentration, with impurity and stability data appropriate to the planned experiment?
The governing framework depends on where the peptide is being studied.
In vitro work centers on reagent identity, assay validity, biosafety practice, and accurate reporting. Animal studies add institutional animal care review, protocol justification, dosing rationale, and humane endpoint planning. Human research introduces a much stricter threshold. Ethics committee or IRB approval, informed consent, adverse event monitoring, and investigational product controls become central. A peptide discussed online for metabolic effects does not become suitable for human use because preclinical papers exist.
Many fat loss articles blur categories. Mechanistic plausibility is not the same as clinical authorization. A receptor pathway may be well described while the peptide itself remains poorly studied, inconsistently manufactured, or unapproved for therapeutic use.
In metabolic studies, safety assessment has to track what changes alongside body weight. Appetite shifts, altered gastric emptying, changes in activity, hydration effects, and lean mass loss can all distort the interpretation of “weight reduction.” If body composition is not measured directly, investigators may mistake a mixed tissue change for selective fat loss.
The muscle-preservation claim deserves particular caution. As noted earlier, reports in this area often overstate how predictable lean-mass retention is. In research terms, muscle sparing is not an assumed property. It is an outcome that has to be measured with validated methods and interpreted in the context of diet, training status, and total energy intake.
A simple analogy helps. Reading only scale weight is like measuring the volume of a chemical mixture without checking its composition. The gross number changes, but the underlying compartments may have shifted in very different ways.
Regulatory discipline in peptide research is partly about subject protection, but it is also about causal inference. If a lab cannot show what material was used, how it was stored, who handled it, and whether adverse effects were monitored under a defined protocol, then both safety conclusions and efficacy conclusions weaken.
At minimum, the section of a protocol dealing with peptide handling should answer four questions:
Those questions sound procedural. They are also scientific. A signaling molecule studied without clear regulatory and safety boundaries can produce findings that look novel but cannot be reproduced or ethically extended.
For research use only, caution is not a disclaimer added after the fact. It is part of the study architecture from the first purchase order to the final interpretation.
A defensible peptide study starts with a narrow question. Broad hypotheses like “Does this peptide improve metabolism?” usually collapse under vague endpoints and uncontrolled variables.
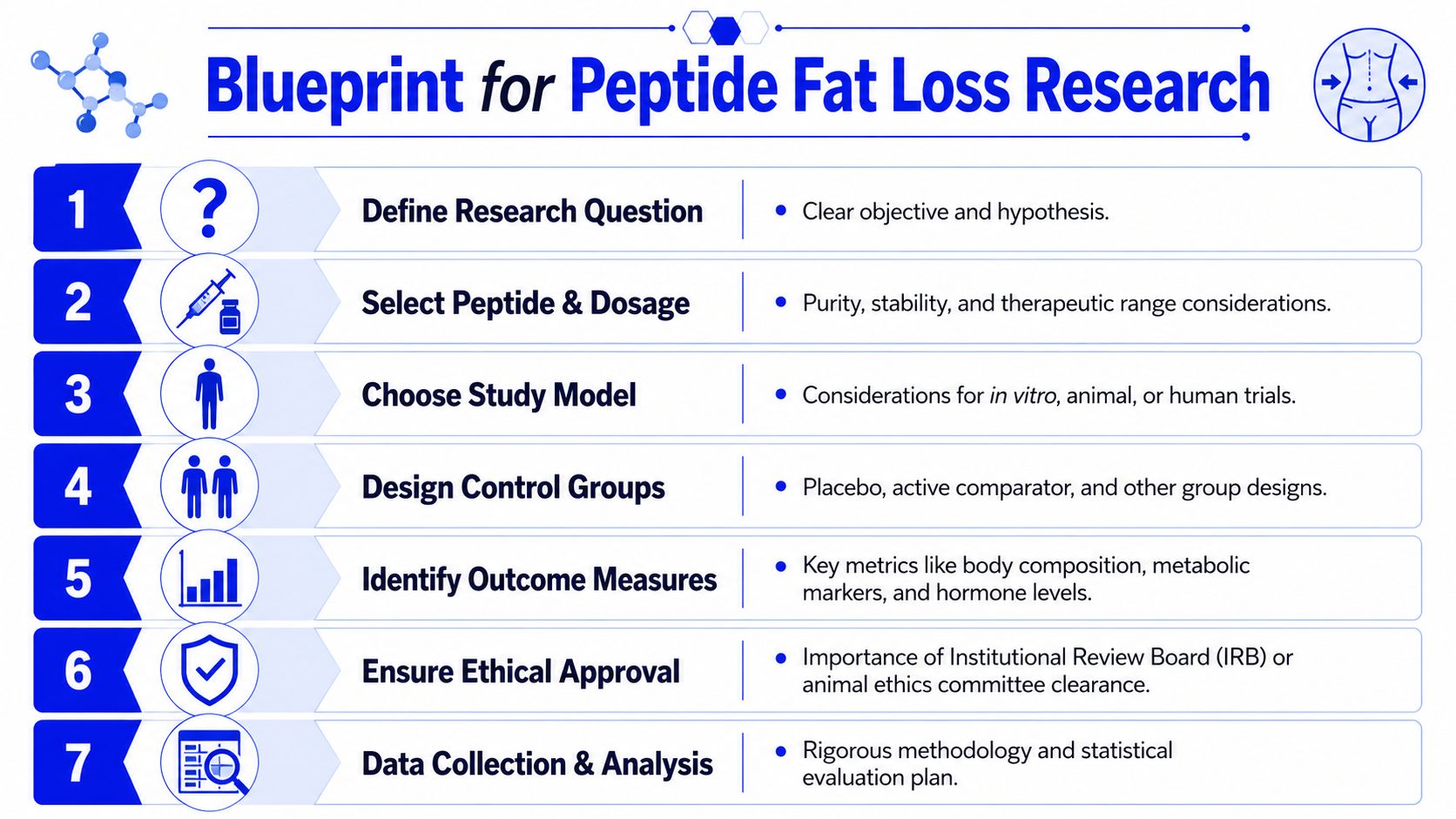
Good research questions are falsifiable. Examples include whether a peptide changes food intake under fixed feeding conditions, whether it alters fat mass relative to a matched control, or whether it changes a metabolic marker without changing total intake.
A useful planning sequence looks like this:
Define the biological target
Choose a receptor, pathway, or metabolic process you can measure.
Select the study model
In vitro, animal, and human literature each answer different questions. Don’t ask a cell model to prove a whole-organism satiety effect.
Specify the comparator
Vehicle controls are often necessary, but some protocols also benefit from an active comparator when pathway overlap is plausible.
The results of many studies can be imprecise. Weight alone is too blunt an endpoint when the compound may affect appetite, fluid balance, gastric emptying, or lean tissue.
Consider tracking a mix of endpoints such as:
Short-term studies may be especially vulnerable to over-interpretation. An early drop in intake can look impressive while telling you very little about durable tissue remodeling.
A clean design usually includes stable housing conditions, consistent feeding protocols, predefined exclusion criteria, and a statistical plan set before data collection starts. Randomization and blinding remain valuable whenever the study model allows them.
A compact checklist helps keep the work rigorous:
The strongest peptide studies don’t just show change. They show that competing explanations were ruled out.
Peptide research in fat loss is promising precisely because it isn’t simple. The most credible compounds act through defined signaling systems, and the most credible studies separate appetite effects, metabolic effects, and body-composition effects instead of collapsing them into a single marketing phrase.
The hard evidence is strongest for GLP-1 related compounds and related metabolic signaling approaches. Outside that zone, many peptides remain better suited to exploratory work than to confident outcome claims. That’s not a weakness of the field. It’s a reminder that receptor biology, dosing context, diet, and tissue-level measurement all matter.
The next phase of research will likely keep pushing toward more selective pathway targeting and better compartment-level analysis of fat and lean mass. For scientists, the practical lesson is already clear. Use high-quality materials, define outcomes carefully, and keep the “research use only” boundary explicit at every stage.
Researchers who want reliable materials for laboratory and preclinical peptide work can learn more at Peptide Warehouse USA. Their catalog focuses on research-use compounds supported by lot documentation, COAs, and batch testing, which can help streamline sourcing when study quality and traceability matter.




Leave a comment